It’s Probably Not Lithium
This post has been recorded as part of the LessWrong Curated Podcast, and can be listened to on Spotify, Apple Podcasts, Libsyn, and more.
A Chemical Hunger (a), a series by the authors of the blog Slime Mold Time Mold (SMTM) that has been received positively on LessWrong, argues that the obesity epidemic is entirely caused (a) by environmental contaminants. The authors’ top suspect is lithium (a)[1], primarily because it is known to cause weight gain at the doses used to treat bipolar disorder.
After doing some research, however, I found that it is not plausible that lithium plays a major role in the obesity epidemic, and that a lot of the claims the SMTM authors make about the topic are misleading, flat-out wrong, or based on extremely cherry-picked evidence. I have the impression that reading what they have to say about this often leaves the reader with a worse model of reality than they started with, and I’ll explain why I have that impression in this post.
(Preamble) A brief summary of their hypotheses
The SMTM authors have recently (a) summarized their hypotheses on how lithium exposure could explain the obesity epidemic. The first hypothesis is that trace exposure is responsible:
One possibility is that small amounts of lithium are enough to cause obesity, at least with daily exposure.
And the second one is that people are intermittently exposed to therapeutic doses:
[E]ven if people aren’t getting that much lithium on average, if they sometimes get huge doses, that could be enough to drive their lipostat upward.
I am going to argue that neither of those is plausible. I address the plausibility of the second hypothesis in the next section, and the plausibility of the first one in the rest of the post.
Lithium exposure in the general population is extremely low, even at the tails, in the majority of countries for which we have data
A few days ago, the SMTM authors published a literature review (a) on the lithium content of food. They conclude that, whereas the existing literature isn’t great, “[i]t seems like most people get at least 1 mg [of lithium] a day from their food, and on many days, there’s a good chance you’ll get more.” They also say it seems plausible that people are intermittently exposed to doses of lithium within the therapeutic range through their diet.
However, their literature review pretty much only includes studies that are outliers in the literature. Moreover, they use a misleading threshold for the therapeutic range of lithium. I’ll explain.
The studies in SMTM’s literature review of lithium levels in food are pretty much all outliers
In 2006, France conducted its second Total Diet Study (henceforth TDS). Across 1,319 food samples, the highest lithium concentration found was 0.6 mg/kg, in water. That’s not the highest average concentration among food groups – it’s the highest concentration of any single sample they tested. (For context, a standard clinical dose of elemental lithium is about 200 mg/day, or 1 gram/day of lithium carbonate.)
Similarly, New Zealand’s 2016 TDS examined 1,056 food samples and the highest concentration it found in any single sample was 0.54 mg/kg (in mussels).
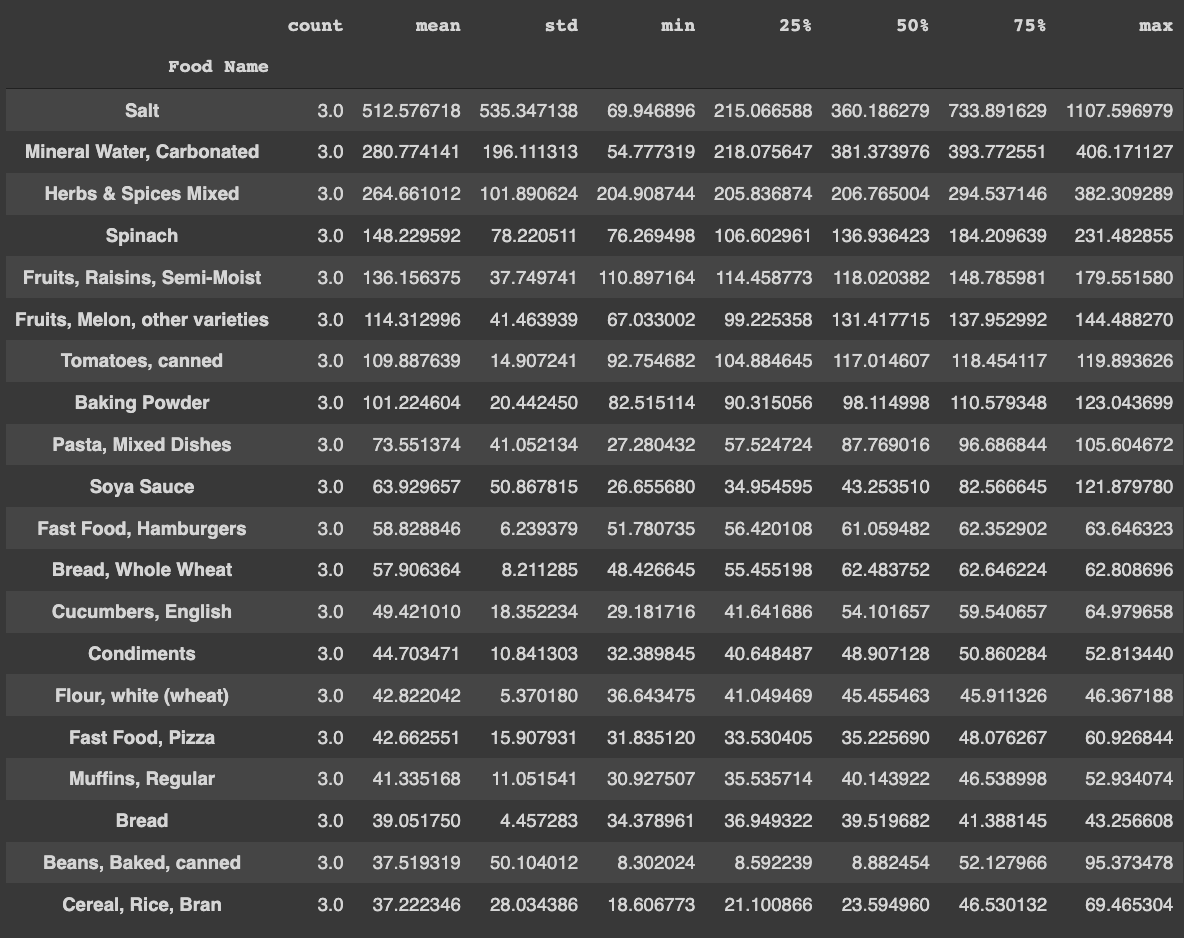
Canada makes the raw data of its Total Diet Study publicly available (a), and they too measure the lithium content of their food. The maximum level reported is 1.1 mg/kg (in table salt, which is presumably rarely consumed in kilogram quantities) across 479 food samples, with the mean being 25 µg/kg and the median 11 µg/kg. Here’s a histogram of the data:
Excluding table salt, the maximum value in the rest of the dataset (N = 476) is 0.4 mg/kg, in mineral water.
Total Diet Studies in other countries report similarly low levels. Using data from the UK’s 1994 TDS (which included 400 food samples), the mean daily lithium intake among adults was estimated to be 17 µg/day, more than 50 times lower than SMTM’s estimate of “at least 1 mg a day”. In Northern Italy, a research group that analyzed 908 samples of food from 2016 to 2017 has estimated that the mean dietary intake is 18.15 µg/day, and an older study in the same area, with 248 food samples, estimated daily dietary intake to be 29.9 µg. Those numbers are similar to estimates from France, which range from 11 µg/day to 48 µg/day, and to estimates from New Zealand’s 2016 TDS, the upper bound of which is 0.31 µg per kilogram of body weight per day, or 31 µg/day for a 220 lb adult.
(Notably, dietary lithium intake in Vietnam, which is extremely lean compared to all other countries mentioned here, is estimated to be 0.285 µg per kilogram of body weight per day, perfectly in line with these other estimates.)
I haven’t been able to find TDS data from other countries. The United States, notably, does not track lithium in its own TDS.[2] But there are a few smaller studies available, neatly summarized by Van Cauwenbergh et al. (1999) (including one from the US, in the last row):
Notice that none of those studies estimates anything as high as “1 mg a day.”
Older sources not included in that table suggest that Finnish diets provide 35 µg/day of lithium, Turkish diets 102 µg/day, and American diets 60-70 µg/day.
SMTM’s review of lithium in food (a) does not include any of these studies; instead, it largely relies on old data from a single author from Germany, a country which, as we can see in the chart above, is a clear outlier. So, unsurprisingly, the numbers that you see in SMTM’s review are way higher than the numbers I found in my own research. The lowest estimate their review even mentions, as a lower bound, for daily lithium intake in the general population, is 128 µg.
To be clear, I don’t think that their data is wrong. It makes sense for lithium concentration to vary a lot in time and space. [3] And whereas the SMTM authors based their literature review mostly on old German studies, the studies I found were from Canada, France, New Zealand, Italy, the UK, Belgium, etc. and a lot of those are very recent. But it is odd that they exclusively talk about outliers, and make conclusions such as “[i]t seems like most people get at least 1 mg a day from their food” based on those outliers.
I have attempted to make a comment on SMTM’s post linking to many of those studies, but they have not approved the comment. I have also attempted to contact them on Twitter (twice) and through email, but have not received a reply. All of this was over one week ago, and they have, since then, replied to other people on Twitter and approved other comments on their post, but haven’t commented on this. So I have no idea why their literature review excludes these studies.
[ETA: on July 5, a week after the publication of this post, they released a post (a) addressing five of the studies I’ve mentioned here (and completely ignoring the rest). I replied to this new post in these comments.]
(Notably, the SMTM authors say in the post that “the smart money is that Anke’s measurements [Anke being the German author most of their review is based on] are probably all lower than the levels in modern food.” If my data from Canada, New Zealand and Italy, all of which is from after 2015, counts as “modern,” then that prediction seems to have turned out horribly wrong.)
Their literature review was misleading in other ways as well; I explain how in my addenda.
People eat about 2 kg of food per day. So it seems that, at least in New Zealand, Canada and France, in order to consume 1.2 mg of lithium in a day you’d need to spend the entire day eating nothing but the most lithium-rich of the 2,851 food samples tested in those three countries combined (excluding salt). And even that value is still 100 times lower than a low therapeutic dose (which, as I’ll explain below, is about 100 mg/day of elemental lithium). So SMTM’s hypothesis that people are intermittently exposed to doses of lithium within the therapeutic range through their diet seems very implausible, at least in those countries (in which, just to make it clear, the obesity epidemic has definitely arrived (a)). [4]
This isn’t, and could not be, conclusive evidence that people don’t intermittently consume therapeutic doses of lithium in those countries. The distribution of lithium concentration in food could be so discontinuous that knowing the maximum value out of the nearly 3,000 samples we have from France, Canada and NZ doesn’t give us much information about what obese people in those countries are likely to have encountered in their lifetime. But the hypothesis that people are intermittently consuming doses that high (at least in those countries) would have to do a lot of work in order to be consistent with our observations.
30 mg/day is not a relevant cutoff
In addition to exclusively mentioning studies with unusual findings in their literature review, the SMTM authors use a subtle sleight of hand to argue that intermittent exposure to therapeutic doses of lithium through food could be the cause of the obesity epidemic. They first say that lithium therapy causes weight gain, citing Vendsborg et al. (1976), in which the average daily elemental lithium dose was 200 mg (SD 8 mg), and also citing this review paper, in which the lowest serum lithium concentration of any patient seems to have been 0.45 mEq/L. Then, later, they claim that the lower end of the therapeutic range of lithium is 30 mg/day, citing a guy on Reddit saying that he takes that much and also has bipolar II, and then they conclude their argument by saying that food could plausibly sometimes contain 30 mg doses of lithium per serving (again, using studies with unusual findings as evidence for this last part).
I say this is a “subtle sleight of hand” because 30 mg/day has doubtful usefulness as a cutoff for a therapeutic dose. As far as I can tell, no patients in the weight gain studies cited by the SMTM authors seem to have been taking a dose as low as 30 mg/day.
Moreover, every (a) source (a) tells (a) you (a) that (a) the (a) therapeutic (a) range (a) of (a) serum (a) lithium (a) concentration starts at ≥0.4 mEq/L (most often ≥0.6 mEq/L) (seriously, just Google “lithium therapeutic range”, the same numbers are everywhere). And unless you’re >65 or have really bad kidneys, 30 mg/day is not enough to get you there – the average adult between the ages of 20 and 65 needs more than three times as much (about 100 mg/day of elemental lithium, or 535 mg of lithium carbonate) to reach 0.4 mEq/L. People over 65 and those with unusually bad kidneys need lower doses, but that hardly helps to explain the obesity epidemic, since people are much more likely to gain weight when they’re young. (Yes, older people do tend to be fatter (up to a certain age) but the rate of change of excess weight is highest in young adulthood.)
Similarly, Googling “lithium dose range” reveals that every single website says that the lowest daily dose is at least 600 mg of lithium carbonate (112.2 mg of elemental lithium), with some (a) sources (a) saying it is as high as 900 mg (168 mg of elemental lithium).
In practice, patient compliance with psychiatric treatment is often not perfect, so there are some people with lower lithium serum concentrations in some studies. However, studies with patients who have low average serum lithium concentrations – under 0.6 mEq/L – seem to find only very modest increases in body weight (or even body weight decreases for patients switching from higher doses)[5]. Moreover, patients with serum lithium concentrations that low experience higher relapse rates, so doctors tend to aim for higher serum lithium concentrations when toxicity is not an issue. The SMTM authors do not address any of that, but rather consistently guide the reader into thinking that a 30 mg/day dose can be expected to lead to therapeutic benefit and weight gain.
(Briefly) Lithium in air and water
The Canadian government has a page (a) with a lot of information about lithium, including concentrations found in the air. From the looks of it, if you breathe outdoor air at the 95th percentile of lithium concentration in Canada, by doing so you will consume 2.86 nanograms of lithium per day. This number is really low, and the numbers for indoor air are even lower, so we probably shouldn’t worry about this. The data we have for the US is similar (though unfortunately, it’s a lot older).
As the SMTM authors have gone into (a), the USGS has measured (a) the lithium concentration of thousands of samples of groundwater in the United States, finding an average of 19.7 µg/L, a median of 6.9 µg/L and a maximum of 1.7 mg/L across 3,140 samples of groundwater from used wells. Values tend to be similar or lower in other countries, except for Chile and Argentina, where they’re much higher.
Importantly, lithium concentrations vary a lot according to lithology and climate, so it seems implausible that people in e.g. humid regions are consuming crazy doses of lithium from their water, as this figure displaying the cumulative distribution of lithium concentrations by climate demonstrates:
(Source: Figure 2 from this paper.)
And this is important, because a lot of the highest-obesity states, such as those in the South, are in humid regions:
Even not taking that into account, however, it seems implausible that a large fraction of the US population is getting therapeutic doses of lithium from their groundwater — even intermittently — given that the maximum concentration across 3,140 samples was found to be only 1.7 mg/L, and given that the average person has only lived for about 15,000 days.
Serum lithium concentration data, just like food data, is strong evidence against the hypothesis that people are exposed to high doses of lithium
First, I’ll give some context for this section. The therapeutic range of serum lithium concentration in adults is 0.4 to 1.2 mEq/L, when measured at the trough, and a higher rate of relapse is described in subjects maintained at <0.6 mEq/L.
The data we have for serum lithium concentration in the general population is probably measured at the trough too (i.e. early in the morning, before people have had any water or food). So with some caveats,[6] it probably makes sense to compare those values directly.
The Canadian Health Measures Survey found that the median whole blood lithium concentration was 0.000068 mEq/L in a nationally representative sample of 5,752 subjects, with data collected from 2009 to 2011. Whole blood lithium concentrations are 65% the value of plasma concentrations (a), which are in turn similar to those in serum, so that corresponds to a serum concentration of 0.0001 mEq/L. This value is 4,000 times lower than the lower end of the therapeutic range, and the 95th percentile (0.00029 mEq/L) is 1,383 times lower.
Given that we have two percentiles, we can estimate the parameters of the underlying distribution, and thus its mean and (e.g.) 99.99th percentile, if we assume that it has a certain shape. Under the assumption that the distribution is lognormal, the average and 99.99th percentile of serum lithium concentrations in that Canadian study are 0.00013 mEq/L and 0.001 mEq/L – respectively, 3,000 times and 400 times lower than the low end of the therapeutic range. This is what the distribution looks like, if we sample from it 100,000 times:
(Feel free to look at my code in this Google Colab notebook.)
If we assume that serum lithium concentration is Pareto-distributed instead, then the 99.99th percentile is 0.0045 mEq/L, still 89 times lower than the low end of the therapeutic range.
The second-largest study of serum lithium concentrations in the general population that I found was this one (N = 928, data collected around 2010 in Germany), in which the median is 0.000138 mEq/L and the 91.7th percentile is 0.0003 mEq/L. Plugging those numbers in the same code, we find a 99.99th percentile of 0.0011 mEq/L in a lognormal distribution and 0.0055 mEq/L in a Pareto distribution, the latter of which is still 73 times lower than a therapeutic dose.
Some places have much higher lithium exposure. In northern Chile, where the highest drinking water concentrations of lithium in the world were found in the 1970s, serum concentrations were only about two orders of magnitude lower than the therapeutic range; a more recent study in nearby northern Argentina, which likewise has extremely high levels of lithium in its rivers, found similar (but a bit lower) levels. And, as we’ve gone into before, some older studies from Germany suggest that lithium levels were quite high in food at the time the measurements were made. Moreover, in the Canary Islands, average dietary lithium consumption has been estimated at 3.7 mg/day.
But I think it’s important to point out this data from Canada, France, New Zealand, etc., because the obesity epidemic is a pretty global problem that has definitely reached those countries, and that is worse in Canada (31% obese in 2016) and NZ (32%) than in Chile (29%), Argentina (29%) or the Canary Islands (20.1%), despite the first two countries having much lower average lithium exposure.
Clinical doses of lithium cause a lot more side effects than just weight gain
But let us suppose for a moment that people are inadvertently taking therapeutic doses of lithium from their food/air/water/whatever every few months or years. There’s still another problem with the lithium hypothesis: why aren’t people getting the other lithium side effects?
Hand tremors
This Cochrane review found that lithium greatly increased the incidence of hand tremors (OR 3.25, 95% CI 2.10 to 5.04; N = 1241; k = 6) among patients taking the drug for a few weeks to control acute mania.
Hypothyroidism
Hypothyroidism is about six times more common in patients on lithium. And notably, its prevalence through time and space doesn’t seem to follow the pattern of obesity. It hasn’t been consistently becoming more common over time, and global rates of the disease don’t seem correlated with obesity rates, with thin countries like China and Brazil having higher prevalences. Moreover, it is more common in old age, whereas weight gain is more common in youth.
Diabetes insipidus
But perhaps the most specific side-effect of clinical doses of lithium is acquired nephrogenic diabetes insipidus.
This disease is not well-known, so I’ll explain what it is. Diabetes insipidus (henceforth DI) is a disease characterized by polyuria (peeing a lot), polydipsia (increased thirst and fluid intake), and abnormally low urine concentration. Polyuria and polydipsia are also found in untreated diabetes mellitus, hence the similar name, but DI has nothing to do with blood sugar.
Most cases of DI in the general population are caused by abnormally low secretion of vasopressin (aka antidiuretic hormone, which gives the signal to concentrate urine); this type is called “neurogenic” or “central.” The type of DI that lithium causes is called “nephrogenic,” and is instead caused by the kidneys becoming unable to respond to vasopressin. Someone with either of those types will pee out a lot of clear urine even after a long period of fluid deprivation — but those with neurogenic DI function normally if they are given desmopressin, so it’s easy to tell those types apart.
Nephrogenic DI seems to be extremely rare in the general population. The NHS website says (a) that the prevalence of any kind of DI is 1 in 25,000, and that DI is nephrogenic in nature in “rare cases.” Acquired (non-hereditary) nephrogenic DI is so rare that lithium therapy is literally its most frequent cause.
How common is diabetes insipidus in patients on lithium therapy? In Vendsborg et al. (1976), 30% of patients had it. Subclinical symptoms of the disease, such as abnormal urine concentration ability, are more common, affecting 54% of 1,105 unselected patients in this study. Notably, the second top post of all time on the r/Lithium subreddit is this (a):
Those symptoms can set in early on with lithium treatment – in Forrest et al. (1974), maximum urine concentration was much lower after 8-12 weeks on lithium than before (Cohen’s d = 3.84, an extremely huge effect size), and such impairment has been found after four weeks of lithium treatment in rats.
It’s true that we don’t know to what extent those side effects happen if you take high doses of lithium intermittently rather than chronically, but note that the exact same argument applies to weight gain.
Weight gain is associated with other lithium side-effects
Moreover, there’s evidence that diabetes insipidus and hypothyroidism might play a role in the weight gain caused by lithium, making it unlikely that lithium exposure in the general population would cause a lot of weight gain in the absence of those other side effects. In Vendsborg et al. (1976), weight gain was much greater among those with greatly increased thirst than among those without:
and much greater among those with clinical diabetes insipidus than among those without:
Vestergaard et al. (1980) report a similar finding. Those studies note that increased thirst can cause weight gain by increasing the consumption of caloric drinks.
On top of that, weight gain is a well-known symptom of hypothyroidism.
(Note: I have attempted to make some of those points in the comment section of SMTM’s last post about lithium, but they never approved my comment. (They did approve some comments made after mine.) There is no mention of diabetes insipidus anywhere on SMTM’s website.)
Even therapeutic doses of lithium don’t cause enough weight gain to explain the obesity epidemic
How much weight gain does lithium even cause, on average? The SMTM authors have cited figures from Vendsborg et al. (1976) and Vestergaard et al. (1980), and I found a number of others (Versteergard et al. (1988), Mathew et al. (1989) and Armond (1996)) in my own research:
All of those studies are observational and none other than the last one has a control group. Patients with bipolar disorder often take antipsychotics and antidepressants in addition to mood stabilizers such as lithium, and the patients in these studies are no exception. In the first two studies, for instance, only a minority of patients were taking lithium alone. Antipsychotics cause weight gain, and the same is true of several antidepressants that were available when those studies were conducted (e.g. TCAs and the MAOI Nardil), so lithium alone probably causes less weight gain than those numbers suggest.
Weight gain does not seem to be constant throughout the duration of lithium treatment; it instead slows down or even stops at some point, as the figures below, from Versteergard et al. (1988) and Kerry et al. (1970), respectively, illustrate:
I mentioned these studies despite their methodological flaws because they have the longest follow-up times I’ve ever found in the literature (and because the SMTM authors cited some of them). What do meta-analyses of RCTs have to say?
I searched Embase for systematic reviews and meta-analyses on the effects of lithium on weight gain, [7]and found 3. This one, from 2012, finds that patients on lithium are almost twice as likely to experience clinically significant weight gain (defined as gaining ≥7% of your body weight) as patients on placebo (k (number of studies) = 5). The two studies that reported patients’ serum lithium concentrations found values of 0.8 ± 0.3 mEq/L and 0.66 ± 0.27 mEq/L; the other studies said that patients were expected to have serum concentrations of at least 0.8 mEq/L.
The second result was a Cochrane Review, which found that people on lithium for acute mania were a bit more likely to gain weight (OR 1.48, 95% CI 0.56 to 3.92; n = 735, k = 3); though the reviewers say that there is “insufficient evidence” that lithium had any effect. This review only included patients in the mental hospital for mania, however, so the average duration of treatment was probably really short.
Oddly, the third result I found was a 2022 systematic review and meta-analysis that says that weight gain during lithium treatment is not statistically significant from zero, and is significantly greater in shorter studies than in longer ones (k = 9, n = 991). Compared to placebo, the meta-analysis finds that lithium causes less weight gain (k = 3, n = 437). I don’t buy this paper’s conclusion, but I think this is nonzero evidence that lithium causes somewhat less weight gain than some other studies suggest.
So lithium seems to cause an average of zero to 6 kg of weight gain in the long term. And strikingly, the upper end of that range, although large, is only half the amount of weight the average American adult has gained since the early 70s, which, according to my analysis of NHANES data (which is all in a public Google Colab notebook) is about 12 kg (~26.4 lb), and as high as 15.7 kg (~34.5 lb) for people in their 30s. (The median American adult gained about the same amount of weight.)
And it’s not as if Americans were that thin in the early 1970s! 47% of adults were overweight and 14.5% obese (a). In contrast, obesity rates are under 3% in traditional societies that engage in foraging or subsistence farming. Moreover, there is substantial (a) evidence (a) that Americans gained a lot of weight before 1970. It’s hard to know the overweight and obesity rates of the general population back in the 19th century, because there was no NHANES back then, but we do know that men at elite colleges (a) (source), Citadel cadets (a) (source) and veterans all started getting substantially fatter in the early 20th century.
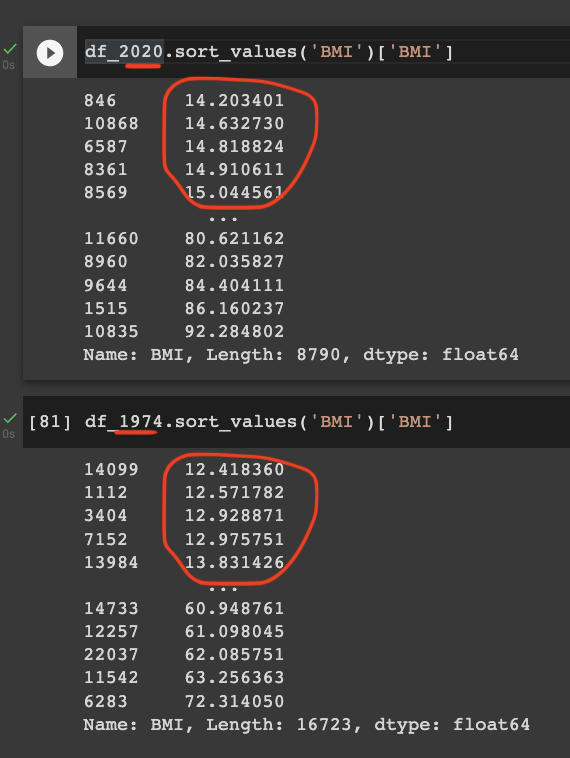
I feel the need to stress this, because the SMTM authors claim (a) that there was an abrupt shift in obesity rates in the late 20th century, a claim that is probably based to some extent on an artifact of the definition of BMI (a), and so some people reading this might have the impression that 1970s Americans were really thin or something, when they really weren’t.
Anyway, so the 12 kg average weight gain since the early 70s is not the whole story. A 5’9” man with a BMI of 21, which is higher than the average for the Hadza (independently of gender or age), for Citadel cadets born in the 1870s, and for men entering Amherst, Yale, or Harvard in the 19th century, is 19.5 kg (43 lb) lighter than the average college-aged American man today. Moreover, a 5’9” man with the average BMI of 19th-century veterans in their 40s is a whopping 22.5 kg (49.5 lb) lighter than the average American man of the same age and height today.
So even if everyone in the US were consuming therapeutic doses of lithium without knowing it, that would leave most of the secular increase in body weight unexplained.
This can also be seen in studies that report the obesity rate or average BMI of patients taking lithium back when obesity rates were low. Chen & Silverstone (1990) (a review article that has been cited by SMTM) reviewed some studies reporting either of those figures, and in none of them was the obesity rate greater than 25% – even though most of those patients were probably on antipsychotics and/or TCAs as well. So it’s difficult to imagine how lithium exposure could explain why the obesity rate is greater than 30% in several countries.
Lithium weight gain seems to (perhaps) be dose-dependent even at therapeutic doses
Furthermore, there’s some evidence that weight gain on lithium is dose-dependent even at therapeutic doses.
Gelenberg et al. (1989) randomized 94 patients on lithium therapy to either a normal or a low dose in a double-blind trial. They found that patients on the low-dose group were about half as likely to report worsening weight gain.
Abou-Saleh and Coppen (1989) likewise randomized 91 patients on lithium therapy to either maintain their dosage or decrease it by up to 50%. The group with the lowest dosage lost 0.9 kg, whereas the highest-dosage group gained the same amount of weight.
Keller et al. (1992) performed the same kind of study, and found that patients in the normal-dose group were more likely to report weight gain than those in the low-dose group.
Moreover, in Vendsborg et al. (1976), one of the observational studies we’ve talked about, there was a 0.44 correlation between lithium dosage and weight gain.
Not all studies find such a dose-dependence – Mathew et al. (1989) did not find one. But the patients in this study had a low serum concentration (0.54 mEq/L on average) and they barely gained any weight (as I’ve mentioned, their average BMI increased by 1 kg/m over the course of 4.7 years). Vestergaard et al. (1980) and (1988) do not find it either. So this seems to be something that might exist, but we’re not sure.
It seems noteworthy, however, that the studies with the best methodology (the first three studies I mentioned, which were randomized double-blind trials) all found dose-dependence. Moreover, when scientific papers say that some association has not been found, often what they mean is that it just hasn’t reached an arbitrary significance threshold. Since Mathew et al. (1989), Vestergaard et al. (1980) and (1988) do not provide any actual data on the amount of weight gained by patients as a function of dosage, for all we know that could be what is going on.
Somewhat relatedly, Rinker et al. (2020) randomized 23 patients with multiple sclerosis to take either placebo or a low dose of lithium (150–300 mg/day of lithium carbonate, ~30-60 mg/day of elemental lithium) for a year in a crossover trial. 13 patients complained of weight gain, but the other 10 complained of weight loss.
Genes that influence BMI do not tend to be expressed in the kidneys (which govern lithium secretion)
If the obesity epidemic were caused by lithium, we should probably expect poor kidney function to predict weight gain, since it strongly predicts serum lithium concentration. But the genes that affect obesity are primarily expressed in the nervous system, and the urogenital system doesn’t stand out at all:
The evidence that trace doses of lithium exert significant effects is actually pretty weak
There’s lots of evidence (or at least, lots of papers) showing psychiatric effects [of lithium] at exposures of less than 1 mg [...]. If psychiatric effects kick in at less than 1 mg per day, then it seems possible that the weight gain effect would also kick in at less than 1 mg.
I’d like to point out that Gwern has looked into this (a) and concluded that the evidence that such low doses of lithium cause psychiatric effects is actually fairly weak.
Mysteries that lithium cannot explain
A Chemical Hunger opens up with a list of mysteries related to the obesity epidemic. I don’t endorse the list – for one, “wild animals are becoming obese” seems to have been pretty much made up (see the fourth point in this comment), and all evidence we have that “lab animals are becoming obese” is exactly one (1) unreplicated paper co-authored by a guy that has been involved in numerous controversies regarding his conflict of interest with the processed food and restaurant industries.[8]
However, some of the mysteries are genuinely true and interesting – for instance, that obesity rates are much lower in high-altitude areas, and that human food is unusually palatable. And lithium does not seem to explain either of those mysteries.
(Note that a theory of the obesity epidemic does not need to explain these mysteries. They could very well be a result of factors completely unrelated to the secular increase in BMI since the early 20th century. But I feel like some people might believe that the lithium hypothesis neatly explains all of SMTM’s mysteries, when it doesn’t.)
Altitude
Using publicly-available data from the USGS and the Open Elevation API, I found that across 1,027 domestic-supply wells (all wells whose coordinates were available), the correlation between altitude and log(lithium concentration) is 0.46. I also checked the correlation between altitude and topsoil log(lithium concentration) in the United States, with data I found here, and, again, it was positive (0.3). So lithium exposure is probably higher, rather than lower, in high-altitude areas in the United States (which, as a reminder, have lower obesity rates).
Palatable human food
To the extent that the mystery is that human food is unusually palatable, and not just that it’s unusually fattening, it’s hard to see how that could be explained by lithium — or any other contaminant, for that matter — being in the food, unless the contaminant happens to be tasty.
Youth (Not mentioned in their blog post series)
As I mentioned before, people gain excess weight much more rapidly when they’re young, at all BMI levels. I think this deserves to be deemed a mystery. And, importantly, it is the opposite of what you would expect if lithium were the cause of the obesity epidemic, because among patients on lithium therapy, controlling for their dosage, young people have lower serum lithium concentrations. In the general population, too, it has been found both in Canada and Germany that serum lithium concentration increases with age.
This doesn’t make the lithium hypothesis impossible – weight gain might be primarily determined by lithium consumption or throughput rather than by serum concentration at any given time. But I think it’s still clearly the case that a positive association between advanced age and weight gain is more likely in worlds in which the lithium hypothesis is true than in worlds in which it is false, and given that the association goes the other way in our world, we should update against the lithium hypothesis accordingly.
Conclusion, bets and bounties
When I imagine a world in which the obesity epidemic is caused by environmental lithium exposure, this is what I expect it to look like:
some places in the Andes and the Canary Islands have way higher obesity rates than everywhere else,
Vietnam has an obesity rate closer to that of New Zealand,
old people are more likely to gain excess weight than young adults,
there is a nephrogenic diabetes insipidus epidemic,
unexplained hand tremors are common,
genes that affect obesity are disproportionally expressed in the kidneys (in addition to the central nervous system),
hypothyroidism rates are going up,
countries and age groups with higher hypothyroidism rates also have higher obesity rates,
therapeutic doses of lithium cause at least ~20 kg of weight gain on average, and
people with chronic kidney disease sometimes mysteriously die of lithium toxicity.
As far as I can tell, none of those things are true. So my credence that lithium exposure plays a major role in explaining the obesity epidemic is very low, something like 0.1%.
Bets
Several months ago, my husband publicly challenged the SMTM authors to a bet on their contamination theory of obesity. They have declined to bet. I’d like to remind them that the bet offer is still active.
Bounties
I am offering a $40 bounty for each Metaculus or Manifold Markets question about the contamination theory of obesity that both I and the SMTM authors agree to be a good test of some aspect of the theory. I’ll pay for up to 5 questions. This bounty expires 90 days after the publication of this post.
I am also offering a $300 bounty for anyone who writes a comment convincingly arguing that the lithium concentration data from the large and recent studies I found from France, Canada, Italy and New Zealand isn’t a good indication of how much lithium people in those countries get from their food, and that it’s actually quite likely that the average dietary intake in those countries is closer to 1 mg/day for a normal-sized adult. Pointing out minor caveats to the interpretation of those studies would not count (though it’s definitely welcome), you have to argue that the data I found is very weak evidence that dietary lithium consumption is on the order of 10-50 µg/day instead of 1 mg/day in those countries. This bounty expires 90 days after the publication of this post.
Right now, whether and to whom this last bounty is paid out is fully up to my judgment. But I am also offering a $50 meta-bounty for whoever comes up with better, objective criteria for that bounty. This meta-bounty expires in 90 days, and if it is fulfilled, then the $300 bounty will expire 90 days after the fulfillment of the meta-bounty.
Update: Austin Chen has offered to match these bounties (in Manifold Markets currency).
Acknowledgments
Thanks to Holly Elmore, Katherine Worden, Philipp Risius, @Willyintheworld and my husband Matthew Barnett for helpful comments and suggestions in earlier drafts of this post.
I do not speak for anyone other than myself, and all errors are my own.
Addenda
Animal products don’t have that much lithium, according to data from France, Canada and Italy
SMTM found, in their food literature review, that animal foods have quite a bit of lithium. They think that that might explain why vegetarian and vegan diets lead to some weight loss. Quoting from their post:
Pretty much everything we see suggests that animal products contain more lithium on average than plant-based foods. [...] It’s interesting, though not surprising, to see such a clear divide between plant and animal foods. In fact, we wonder if this can explain why vegetarian diets seem to lead to a little weight loss and vegan diets seem to lead to a little more, and also why neither of them work great.
However, this horribly fails to replicate in the Total Diet Studies that I’ve found in my research. For instance, the food item with the highest lithium concentration in the second French Total Diet Study is… definitely not something that vegans are known for not eating:
The first French Total Diet Study likewise found that meat (2 µg/kg), milk (6 µg/kg) and ultra-fresh dairy products (4 µg/kg), among other animal foods, had a lot less lithium than fruits (7 µg/kg), vegetables (14 µg/kg), miscellaneous cereals (20 µg/kg), nuts and oilseeds (22 µg/kg), and Viennese bread (37µg/kg), among other plant-based foods.
Moreover, in the Canadian TDS (a), all of the top 10 foods in average lithium concentration are vegan, as are all but 3 of the top 20, as you can see in this Google Colab notebook:
In the large Italian study I have mentioned before, the highest lithium concentration was found in fish/seafood (median 19.10 µg/kg) (the same finding as the first French TDS) but legumes (15.43 µg/kg) and cereal (14.83 µg/kg) also had a lot of lithium, whereas meat products (3.41 µg/kg), eggs (3.87 µg/kg) and dairy products (4.78 µg/kg) all had low levels. This other study from Italy found that fruits and vegetables (33 µg/kg) and cereals and tubers (31 µg/kg) were the food groups with the highest lithium concentrations.
So it doesn’t look at all like there is a “clear divide” between plant and animal foods.
We *do* have data on the lithium content of processed food
Again from SMTM’s literature review of the lithium content of food:
One thing we didn’t see much of in this literature review was measurements of the lithium in processed food.
We’re very interested in seeing if processing increases lithium. But no one seems to have measured the lithium in a hamburger, let alone a twinkie.
Fortunately, this is incorrect — Canada has measured the lithium in hamburgers, and the concentration they found was 58.8 ± 6.2 µg/kg. They also measured the lithium content in pizza (42.66 ± 16 µg/kg), French fries (26.77 ± 20.8 µg/kg), hot dogs (25.49 ± 3.9 µg/kg), chicken nuggets (10.78 ± 3.4 µg/kg), fried rice (12.11 ± 2.8 µg/kg), prepackaged sandwiches (27.14 ± 1.3 µg/kg), and other types of fast food.
France, too, has measured the lithium concentration of a variety of processed food items, in its first and second Total Diet Studies.
Factual inaccuracies and misrepresentation of sources in SMTM’s posts about lithium
Since we’re already here, I decided to point out and correct a few claims that the authors of SMTM have made in posts about lithium that are not supported by their own sources.
No, Texas counties with higher lithium levels are not more obese
In Part VII: Lithium (a), the SMTM authors say:
In Texas, a survey of mean lithium levels in public wells across 226 counties (Texas has 254 in total) found lithium levels ranging from 2.8 to 219.0 ng/mL. Now Texas is not one of the most obese states — but it tends to be more obese along its border with Lousiana [sic], which is also where the highest levels of lithium were reported.
However, if you look at the source, their map of lithium levels across Texas counties actually says the opposite – that counties along the border with Louisiana have lower lithium levels than other counties (though it’s a bit confusing because on the map darker areas represent lower levels):
Someone else has already pointed this out in the comments of that post, several months ago, as have I, on a 05/08/2022 Twitter thread tagging the SMTM authors, but the post has not been fixed, and the authors have not acknowledged or addressed the error in any way.
When you calculate the correlation between log(water lithium levels) and log(obesity %) in Texas, you find that it is −0.13.
No, obesity in the West Bank was not 50% in men in 2003
Also from Part VII: Lithium (a):
obesity in the West Bank is pretty high — as high as 50% in men in 2003!
Again, that is not supported, but is instead contradicted, by the authors’ source. It says:
The prevalence of obesity was 36.8 and 18.1% in rural women and men, respectively, compared with 49.1 and 30.6% in urban women and men, respectively.
I pointed that out in a comment, but they have not edited their post.
No, you did not find hints that people on Samos Island are about as obese as Americans
From Interlude H: Well Well Well (a):
in our first post on lithium, we found hints that people on Samos Island are about as obese as Americans.
Their first post on lithium (a) in turn says:
In Greece, lithium levels in drinking water range from 0.1 ng/mL in Chios island to 121 ng/mL on the island of Samos, with an average of 11.1 ng/mL. Unfortunately there’s not much data on the prevalence of obesity in Greece, but we can conduct some due diligence by checking a few of these endpoints. Samos, with the highest levels, is the obvious place to start. On Samos, 10.7% of children aged 3-12 are overweight, compared to 6.5% on the island of Corfu. A full 27% of high schoolers on Samos island were overweight in 2010, and 12.4% were obese. In comparison, about 12.5% of American high schoolers were obese in the same period.
The comparison with American high schoolers in that paragraph is not appropriate. The US uses a different method for defining childhood obesity than the rest of the world. Remember that the definition of obesity in adults (BMI ≥ 30 kg/m) is a bad fit for children and adolescents, who tend to be naturally thinner, so obesity cutoffs are rather defined by percentiles. And whereas the US uses cutoffs based on data from American children (a), the Samos island paper uses cutoffs adopted by the International Obesity Task Force, which are different.
I have attempted to point this out by making a comment on their post, but they have not approved the comment.
Moreover, Chios and Samos, despite their very different drinking water lithium levels, have rather similar obesity rates: 10% of teenagers in Chios are obese and 25.5% are overweight.
(Added on July 7, 2022) No, dry weight is not the same thing as fresh weight
In a post (a) that was published a week after this one (and which I address in these comments), the SMTM authors say the following:
Hullin, Kapel, and Drinkall (1969) found more than 1 mg/kg [of lithium] in salt and lettuce, and up to 148 mg/kg in tobacco ash. [...] Magalhães et al. (1990) found up to 6.6 mg/kg in watercress at the local market.
They present those studies as contradicting the Total Diet Studies I’ve found (which report usually a few tens or hundreds of micrograms per kilogram of lithium in food) but fail to mention that both Hullin, Kapel, and Drinkall (1969)‘s estimate of lithium concentration in lettuce, and Magalhães et al. (1990)’s estimate of lithium concentration in watercress, had the dry weight of those plants as the denominator, not their fresh weight. This is important because both of those plants are known to be 90%+ water by weight, and Total Diet Studies report lithium content per unit of fresh weight, so those estimates are not at all comparable.
Later on in the post, they claim that some food in Brazil has more than 1 mg/kg in lithium concentration, a claim that is probably based on Magalhães et al. (1990) (the only study they cite that seems to be from Brazil), and use that as evidence that the Total Diet Studies are wrong. And, again, that is very misleading. The very paper they cite explicitly estimates that you would need to eat 400 g of watercress per day to consume 70 µg/day of lithium (unless you go out of your way to feed more lithium to those plants as they’re growing, which is an experiment they report in the paper), which implies a fresh weight lithium concentration of 175 µg/kg.
I have asked them on Twitter to fix this, and they haven’t yet.
Relatedly, several of the other estimates of high lithium concentration in food that they mention have dry weight as the denominator (those from Borovik-Romanova (1965) and those from Ammari et al. (2011)), but they nevertheless present them as contradicting Total Diet Studies.
Errata
I had originally failed to specify that the dose given to patients in Rinker et al. (2020) was 150–300 mg/day of lithium carbonate (~30-60 mg/day of elemental lithium). I fixed this around 8:40 PM Pacific Time on 06/28/2022 (the day of this post’s publication.)
- ^
They also think that other contaminants could be responsible, either alone or in combination.
- ^
The SMTM authors point out that one of their sources cites a 1985 EPA estimate that dietary lithium intake among Americans is 0.650 to 3.100 mg per day. However, the original source cannot be found, and this 1995 article on the EPA’s website about environmental lithium exposure makes no mention of such an estimate. It instead says,
A wide range of estimates for daily dietary intake of lithium has been reported. Several authors report estimates for the average daily dietary intake of lithium, ranging from 0.24 to 1.5 μg/kg-day (Noel et al., 2003; Clarke et al., 1987; Hamilton and Minski, 1973; Evans et al., 1985; Clark and Gibson, 1988). A much higher estimate for daily intake from food and municipal drinking water ranging from 33 to 80 μg Li/kg-day was reported by Moore (1995).
Moore et al. (1995) in turn seem to base their estimate of dietary lithium intake on Bowen (1979) (page 253), which estimates the following concentrations of lithium in living tissue (in mg/kg of dry matter): “Land plants: 0.5-3.4. Edible vegetables: 0.8-1.3. Mammal muscle: 0.023.” These estimates are substantially older than ~all of the other ones I’ve found, and their country of origin is unclear.
Moore et al. (1995) then multiply those numbers by the amount of mass from each of those types of tissue that people consume on average per day (“0.34 kg meat, 0.39 kg dairy products, and 0.76 kg vegetable and grains,” according to the USDA).
The USDA report does not indicate that those are numbers for dry matter consumption. So Moore et al. (1995) seem to be multiplying the lithium concentration in dry matter by the mass of fresh matter of each type of food that people consume per day, if I’m understanding correctly. If that is what is going on, Moore et al. (1995)’s numbers substantially overestimate dietary lithium consumption, since fresh mass tends to be a lot greater than dry mass for a lot of foods.
- ^
They can also vary depending on the method used to make the estimate. Schrauzer (2002) mentions a lot of unpublished, very high (but still mostly < 1 mg/day) estimates of dietary lithium intake that are based on hair concentration rather than actual measurements of lithium in food.
Interestingly, the highest estimate this source mentions is for people in China, a country famously known for its devastatingly high obesity rate.
- ^
Let’s examine the matter more quantitatively. The SMTM authors think that the distribution of lithium concentration in food is lognormal (a). Since we have Canada’s raw data, we can estimate the parameters of the lognormal distribution by using scipy.stats.lognorm.fit (a). Doing so, I estimate that 1 in 1,000,000 food samples in Canada has more than 3.2 mg/kg of lithium. Human life expectancy is about 30,000 days, and people probably don’t consume more than 33 different food items every day, so this is more than a person would realistically encounter in a lifetime.
How well does that model fit the data? Running a Kolmogorov-Smirnov test reveals that it’s quite a good fit, and a way better fit than the heavier-tailed Pareto distribution. But if we want, we can ditch the assumption that the distribution is lognormal, and use kernel density estimation instead. Doing so, I estimate that 1 in 1,000,000 food samples have more than 1.1 mg/kg of lithium, when I use the default parameters of sklearn.neighbors.KernelDensity.
- ^
Note, however, that I’ve found only a few studies in which the average serum concentration was that low.
- ^
The caveat is that patients on lithium therapy may have higher trough levels as a fraction of their peak levels.
So how should we adjust the data, in light of that? It seems, from lithium pharmacokinetics studies, that 24 hours after a single high dose, serum lithium concentration should be only two to six times lower than it was at its peak. Lithium might be cleared more rapidly at lower levels, for all we know, so these data must be interpreted in context – with food, water and air lithium concentration data in mind.
- ^
My search string was “lithium:ti AND ‘weight gain’:ab,ti AND ([cochrane review]/lim OR [systematic review]/lim OR [meta analysis]/lim)”. Embase requires institutional access; if you don’t have that you can search PubMed instead, which, like Embase, allows you to restrict your search to systematic reviews and meta-analyses. PubMed has fewer studies than Embase, but for this specific query it yielded the same relevant results.
- ^
The guy is David B. Allison. I’d care less about the conflict of interest if that paper had ever been replicated at all, but it hasn’t. Moreover, a few months ago, I investigated whether the most popular strain of lab mice has been getting more obese since 2000, using publicly available data, and found that it hasn’t.
- (The) Lightcone is nothing without its people: LW + Lighthaven’s big fundraiser by (Nov 30, 2024, 2:55 AM; 610 points)
- Luck based medicine: my resentful story of becoming a medical miracle by (Oct 16, 2022, 5:40 PM; 490 points)
- On not getting contaminated by the wrong obesity ideas by (Jan 28, 2023, 8:18 PM; 306 points)
- My Effortless Weightloss Story: A Quick Runthrough by (Sep 30, 2023, 11:02 PM; 124 points)
- Voting Results for the 2022 Review by (Feb 2, 2024, 8:34 PM; 57 points)
- 2022 (and All Time) Posts by Pingback Count by (Dec 16, 2023, 9:17 PM; 53 points)
- Potato diet: A post mortem and an answer to SMTM’s article by (Jul 14, 2022, 11:18 PM; 48 points)
- Experimental Fat Loss by (Jun 1, 2023, 8:26 PM; 23 points)
- 's comment on Thoughts on seed oil by (Apr 22, 2024, 1:50 AM; 5 points)
- Uncursing Civilization by (Jul 1, 2024, 6:44 PM; -5 points)

This post publicly but non-confrontationally rebutting an argument that had been put forward and promoted by others was a tremendous community service, of a type we see too rarely, albeit far more often in this community than most. It does not engage in strawmanning, it clearly lays out both the original claim and the evidence, and it attempts to engage positively, including trying to find concrete predictions that the disputing party could agree with.
I think this greatly moved community consensus on a moderately important topic in ways that were very valuable. I will note that it’s unfortunate but indicative that SMTM never responded.