Reporting in the wake of Christmas remains spotty, but this fog of war was anticipated, and we must do what we can with what we do know. Mostly, what we’ve learned reinforces the picture outlined in Post #9, with reduced severity. Also with reduced generation time which we confirmed a bit via a study from South Korea.
I’ve also written up Omicron: My Current Model which gives the ‘here’s where we are at’ takeaways and news you can most practically use.
Denmark
Denmark’s reporting is usually excellent, but they’ve taken a few days off for Christmas and I don’t see new data even now, so nothing new to report on that front.
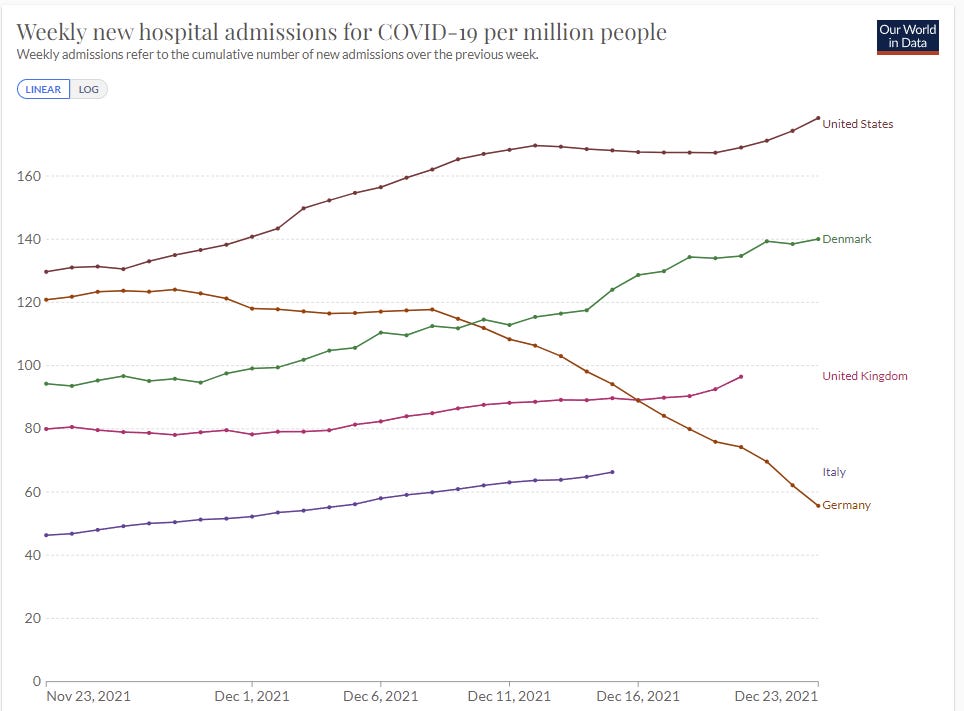
Hospitalizations continue to come in lower than expected (WaPo).
More important, hospitalizations have come in — so far — on the very low end of what was projected. A week ago, Denmark’s government science institute said daily new coronavirus hospital admissions could range between 120 and 250 patients by Christmas Eve. In recent days, daily admissions have hung around 125.
That’s not a big range, only varying by a factor of two. It reflects a kind of overconfidence – we have large uncertainty over true case counts and over severity on multiple fronts. We have known cases increasing by a factor of three or four depending on how you count lag, real cases doubtless up far more than that, yet hospitalizations only up about 50%, and still solidly below the United States.
The UK’s hospitalization numbers here are less promising, because given the delays in reporting plus lag in events, we still don’t have much information.
By Thursday data should have caught up, and we’ll have a strong data point on the severity level of Omicron. We won’t know if cases peaked or not, because of the holidays, unless the numbers kept going up in spite of the holidays.
United Kingdom
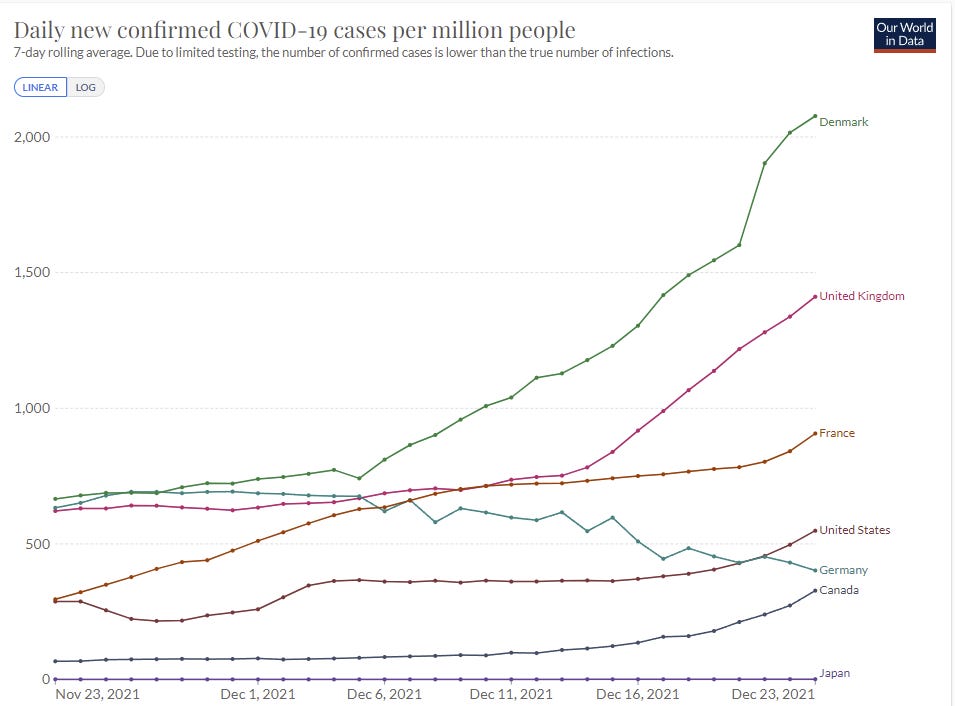
Looks like cases continue to rise, but holidays again make it very difficult to be certain.

The temporary drop in testing followed by a return to trendline indicates to me that it was a temporary blip. It may have been reluctance to test, or reduced testing capacity, before the holidays. It may have been behavior change in advance of the holidays. Either way, records are once again being set.
Another data source and perspective.

There’s no way we had this kind of decline that quickly given subsequent data. The only plausible interpretation here is that people stopped reporting.
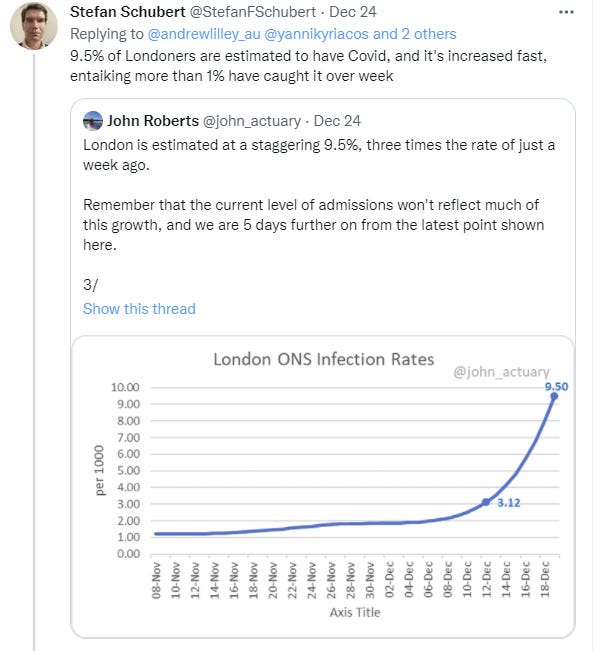
Another estimate has 9.5% of Londoners Covid-19 positive on Christmas Eve, which seems plausible to me.
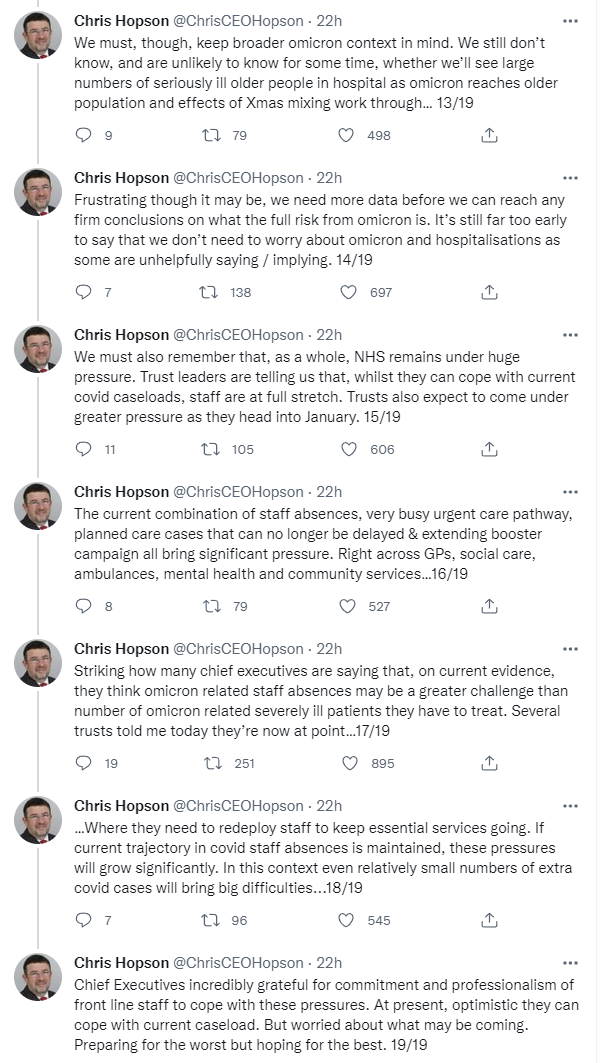
Thread on UK hospital situation. Important questions here so quoting in full for those interested.
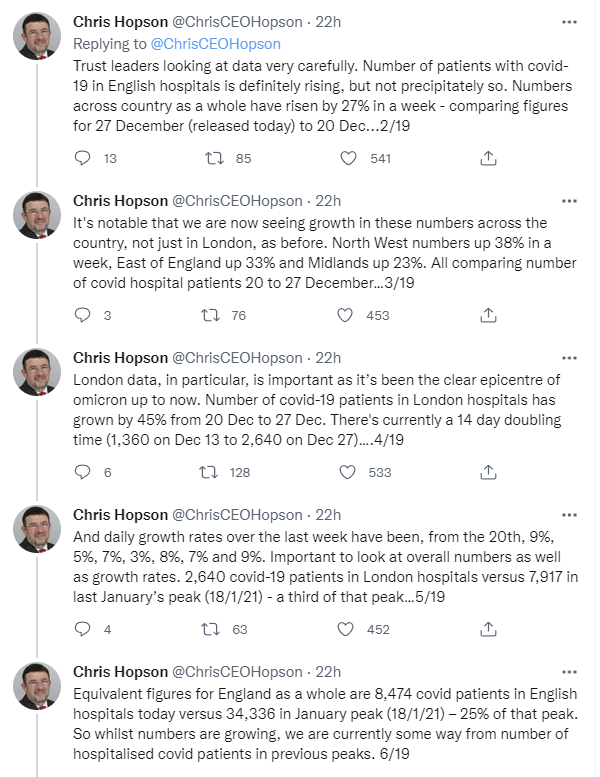
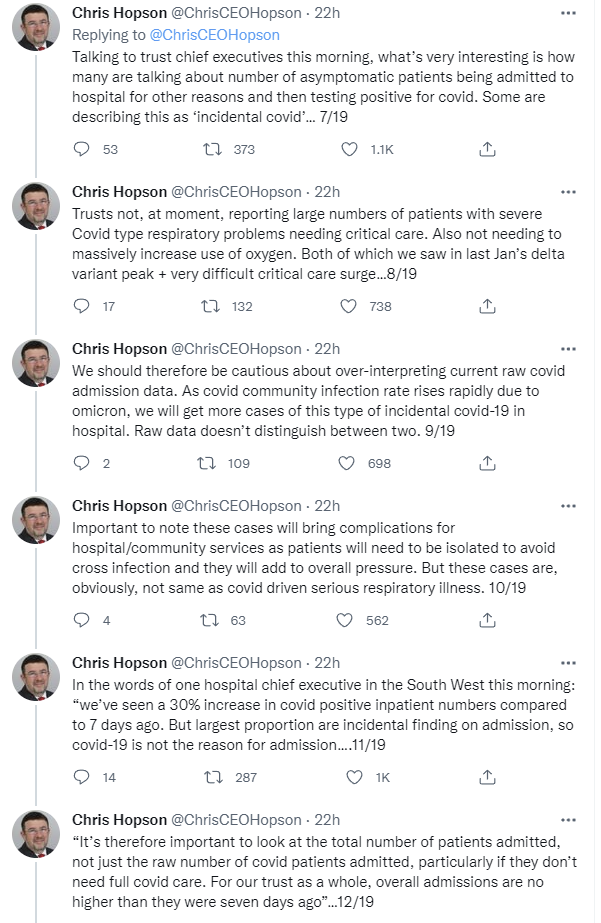
I find #12 especially interesting here: We don’t know which patients are in the hospital because of Covid, and that’s what matters, so ideally we’d compare total admissions now and then, the same way we might measure net excess deaths. As long as there’s plenty of capacity, that seems right, but the obvious problem is that as hospitals fill up admission criteria changes, and once they’re full admission numbers are effectively a constant, so this metric breaks down rapidly under strain. But if overall numbers haven’t changed at all, and there was capacity before, that seems like a big game. Then again, #15 notes that NHS was already under tremendous pressure. If anyone reading this works at a UK hospital, especially in London, I’d ask, if you know: Are the thresholds for admission starting to rise? Or are you using the same heuristics you were last month? And are the staff shortages pushing down ability to admit patients and reducing admissions that way?
So we can’t draw firm conclusions, as Hopson notes, but it’s still promising news. It certainly seems at this point to rule out relatively horrible outcomes on severity. By this point we would know.
Around the World
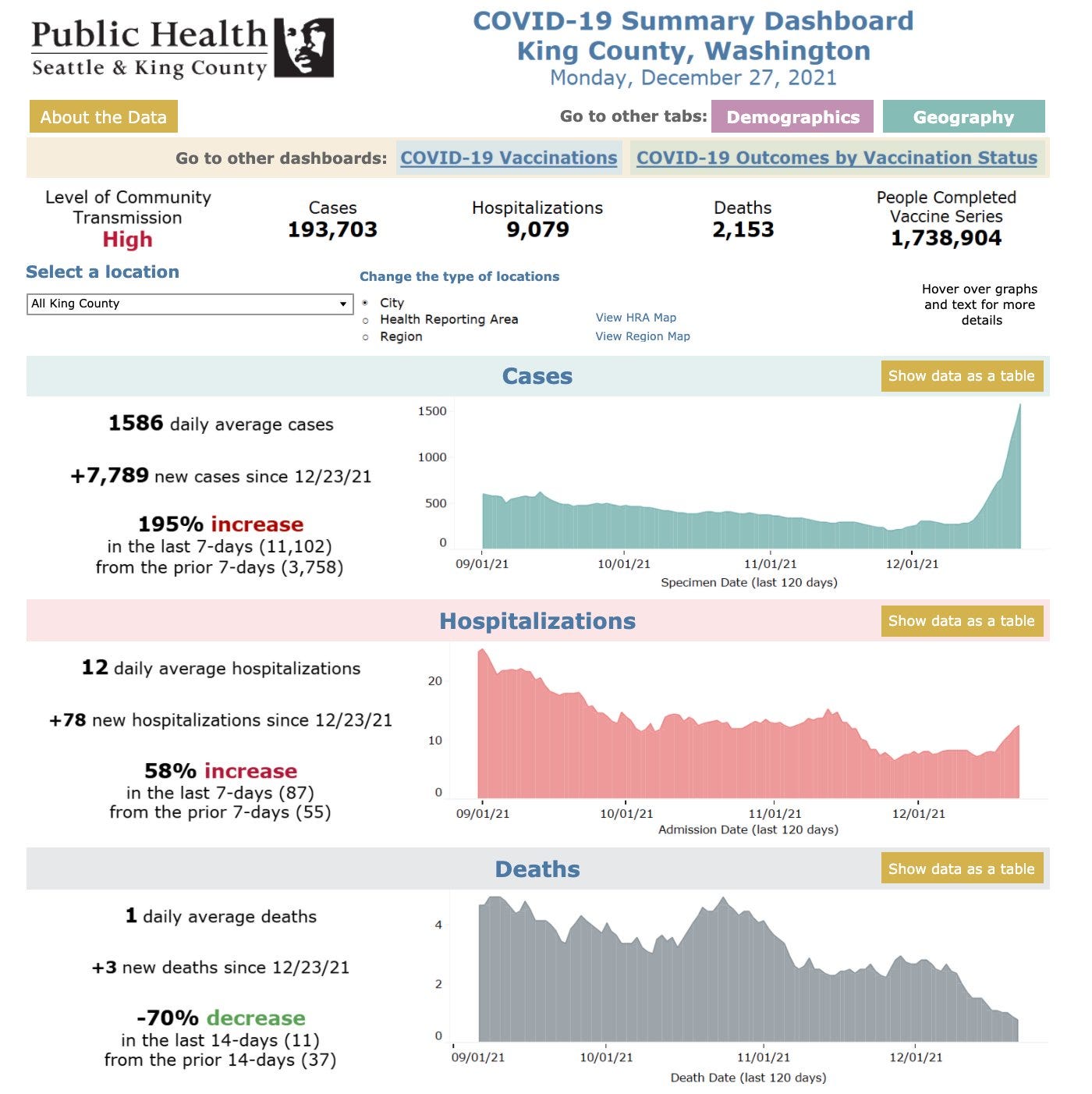
Washington State at 95% Omicron several days ago. So far, hospitalizations are rising much slower than cases, but lag makes it hard to know yet.
Rolling Stone assumes New York City is going to be okay because of high vaccination rates, but worries others won’t be because of lower rates, because the universe to such folks is a morality tale. New York needs its stronger prevention methods because it is naturally a much riskier place to be in a pandemic than most other places, the same way London is.
New York’s case count set another record over the weekend by a wide margin, even dividing the two-day report over two days. So far it’s not translating into a crisis, and at current rates things will be over fairly soon, but it’s a rather scary place to be.
Germany seems to be stopping Omicron in its tracks. Hospital admissions are down and cases are also down. I notice I am confused here. Germany’s rate of improvement under Delta wasn’t that rapid, so it shouldn’t have been sufficient for Omicron beyond slowing things down somewhat.
Nowcast Update
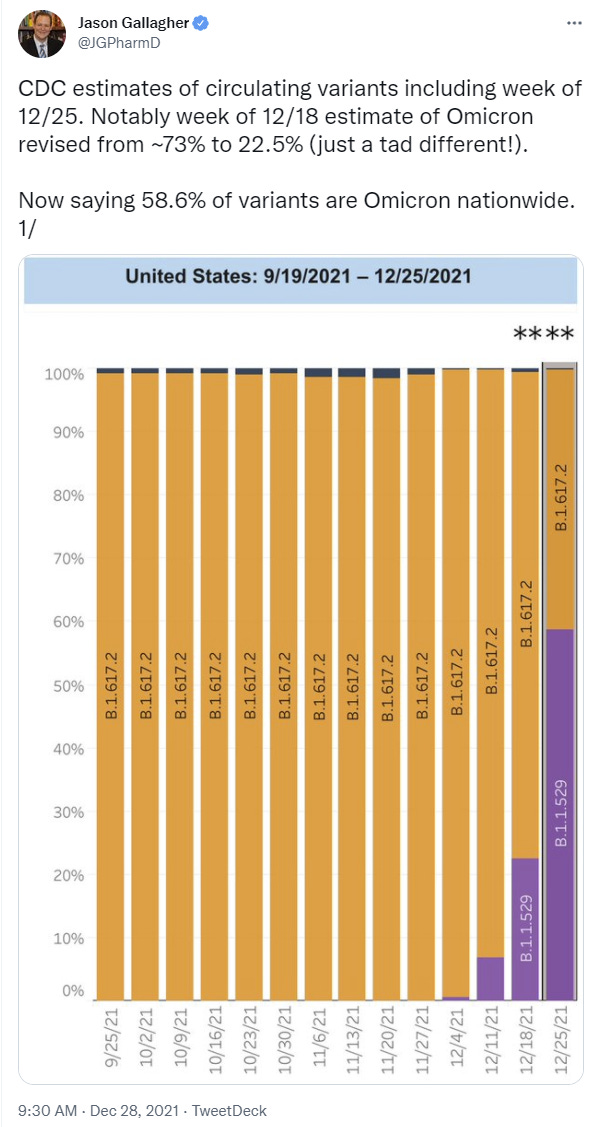
When the CDC came out with its nowcast update last week saying Omicron was 73% of cases and 95% of some areas, I noticed I was confused, eventually devoting a post to the question. I concluded that the nowcast was on the fritz, its model unable to handle the out-of-sample conditions being presented to it, and it was spouting out obvious nonsense that conflicted with many other data points.
It looks like that was correct, given the huge revisions we see this week. 73% is now 22.5% (!) and even this past week they only have us at 58.6%.

Agreed that little actual damage got done, treatment wasn’t impacted and mostly people didn’t pay the 73% number much mind. The new numbers are more reasonable, but seem low. We should expect a more rapid takeover than this, given large penetration in all geographical areas, so I think Nate’s take here is correct.
It’s good and right to revise numbers and admit you’re wrong, and the error here isn’t as big as it looks because exponential growth makes fools of us all. Still. When things are moving rapidly, the CDC’s methodology extrapolates in ways that make it highly unreliable, and we’re better off ignoring it.
Severity
Japanese preprint (direct link) claiming that Omicron has reduced binding potential to the lungs, and it is likely more transmissible but less pathogenic.
Abstract
The emergence of a new severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2) variant, Omicron, is the most urgent concern in the global
health in December 2021 (ref.1). Our statistical modelling estimates that
Omicron is >3.0-fold and >5.6-fold more transmissible than Delta in South
Africa and the UK, respectively. Intriguingly, cell culture experiments show
that Omicron is less fusogenic than Delta and ancestral SARS-CoV-2.
Although the spike (S) protein of Delta is efficiently cleaved into the two
subunits, which facilitates cell-cell fusion2, Omicron S is faintly cleaved.
Further, in hamster model, Omicron poorly infects and spreads in the lung
and is less pathogenic compared to Delta and ancestral SARS-CoV-2. Our
data suggest that the efficacy of SARS-CoV-2 S cleavage and viral
fusogenicity are closely associated with viral pathogenicity, and Omicron
evolved to exhibit increased transmissibility and attenuated pathogenicity.
I’m insufficiently knowledgeable to evaluate these claims easily, but this isn’t the first result of this type, or the first similar interpretation.
Spread
South Korean study from 25 December estimates serial interval (generation time) of Omicron in South Korea at 2.2 days (!) +/- 1.62 days with R0 = 1.6. With that low a generation time 1.6 is still going to add up mighty fast. Note that 2.2 days is mind-blowingly low. If that’s a mean, then it implies that most of the spread is within four days of exposure. By contrast, a similar study of Delta found 3.3 days as the generation time, which is also much faster than the standard assumption of 5 days.
This isn’t a big enough sample to gain too much confidence, but it’s additional evidence in favor of shorter generation times.
The study also notes that 31% of cases at the church where the incident took place were double-vaccinated people, whereas 80% of the Korean population is double vaccinated, but they did not check for vaccination status at the church overall, which could easily have had a lower vaccination rate, so I wouldn’t read much into that.
I’ve heard of the CDC and similar government statements being overly conservative, but this seems rather ridiculous.

But the CDC said “scenarios with lower immune evasion” predict that the surge “could be lower and begin as late as April 2022.”
The report was updated on December 20. Here’s their ‘scenarios:’
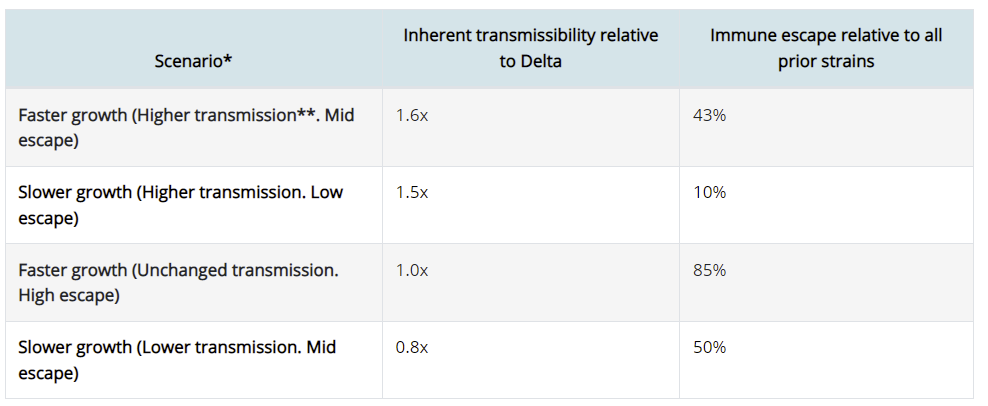
Yeah, none of these are plausible scenarios, or were plausible on December 20th.
Threads and Posts
Noah Smith Christmas Omicron Update. Reaches similar conclusions to post #9.
Stat News overview, and I have to admire the headline.
Always curious is where they try to take an exponential and make it linear somehow, without doing the math I’d think you had to do. In this case it’s here.
The newest variant has also inexorably altered the course of the pandemic. Although it’s still unclear how high and how fast the curves will climb (and how many people will get very sick or die in the process), Murray said when he and his team run their models further out, they see Covid-19 quieting down for much of 2022. “The thing Omicron will do, because it’s going to infect 40% of the entire world in the next two months, is it will raise population-wide immunity for a while,” he said. After a massive Omicron wave passes through, transmission should drop to very low levels. Ongoing rollouts of vaccines should help keep it that way.
Numbers like the 40% here always make me wonder, and I’m always sad to see people feel the need to say ‘for a while’ after such statements. Why should it stop at 40%? Why would 40% be sufficient to drop transmission to ‘very low levels’ given what we know?
There’s also the usual raising of possibilities that have already been mostly ruled out, but overall it’s not bad, better than expected.
For what the rhetorical case for panic looks like, 23 December thread from Yaneer Bar-Yam claiming high severity. Uses the ‘but Long Covid’ move and the ‘children are dying’ move based on reports of 21 deaths, which he says is a 3.5x increase and 3% of deaths (the discussion that follows involved a bunch of questioning of that claim and its source), calls for ‘protecting kids’ and ‘everyone’ from Omicron as if that is a thing that one could do. Even if fully accurate and representative (I have my doubts), that’s still 3% of deaths in kids that make up 34% of South Africa’s population, and that are presumably almost entirely unvaccinated, and out of a much reduced number of deaths versus previous waves. It’s clear he, like many others, interprets ‘severity’ as ‘the thing we want people to think is high.’
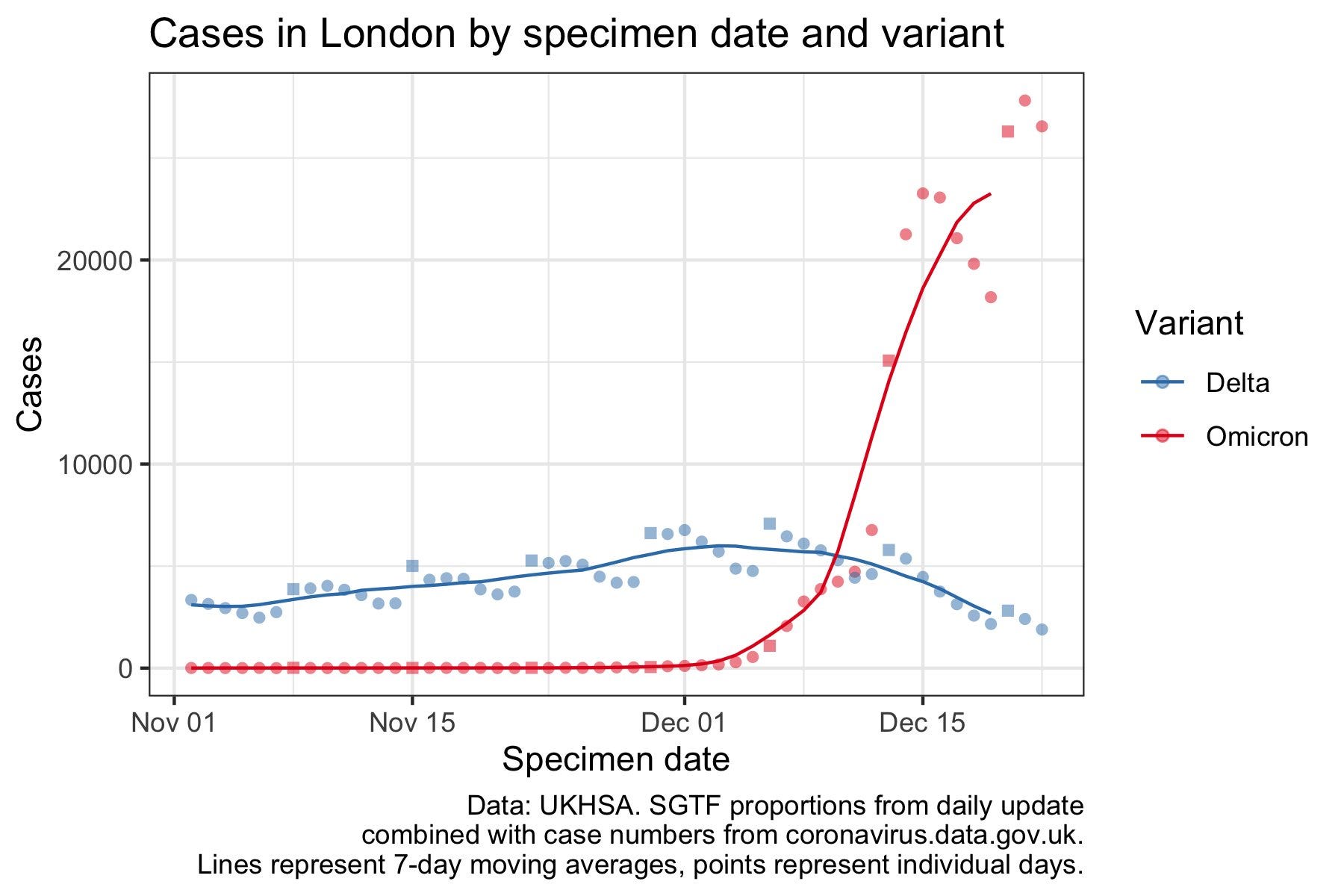
Trevor Bredford thread from 23 December viewing London as having peaked, with a (corrected) estimate of 10% of Londoners having had Omicron so far, or about triple the official number. I find that implausibly low, especially if the peak was real.
This thread from Farzad Mostashari estimates that about 3% or fewer of NYC Omicron patients likely end up needing hospitalization, which makes sense to me, in fact I think this underestimates case counts quite a bit and it’s even lower than that. Where I get confused is where suddenly he says this:
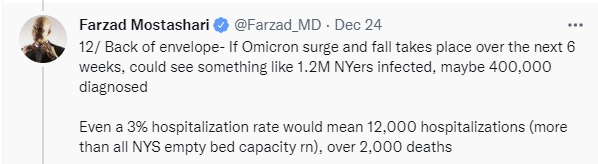
It would be profoundly surprising to have only a 15% or so infection rate for Omicron, especially given other ways of doing estimates, such as the situation where NYC faces a shortage of EMS crews.
Roughly 19% of the city’s more than 4,000 EMS workers were out sick Saturday, Christmas day, up from the typical rate of about 5%, an FDNY spokesman said.
The shortage — caused in part by crews isolating with COVID-19 cases — comes as the city’s daily number of cases continued a record breaking streak.
The question is, is that 19% of workers who were themselves sick or was that 19% who were sick or isolating due to exposure? As written it’s the first one, and it suggests a 14% rate of Covid infection, many times the citywide officially reported rate. I am inclined to believe the 14% rate, and to use it as a baseline for where things are in NYC. The 5% ‘normal’ rate seems higher than the usual baseline for sick days, and also presumably people are calling in sick with other non-Covid things more aggressively on the margin, but then again surely some people don’t notice they’re positive or power through it, so it’s not obvious the right direction to adjust this.
Certainly 15% already having gotten Omicron seems more plausible than 15% being the stopping point after six weeks. We’re already seeing official tallies of 0.3%/day, which is almost 15% found cases after six weeks of that, and that somehow assumes no further doublings.
Other News
Confirmation that Omicron infection protects against Delta. I wasn’t worried about this but it’s always good to have confirmation.
A lot of flights are getting cancelled, here’s one report of many. I had a visitor last night because his flight was delayed several times, leaving him time to come into the city, and he had to ultimately leave at 2:30am.
As a reminder, it’s quite the outlier, Omicron really does have a huge number of mutations.
Josh Barro points us to CDC statistics on infections on cruise ships, he says that a majority of ships reporting infections is new. My understanding was that for a while every cruise ship was automatically Covid-infected, and thus we stopped having cruise ships, but that wasn’t based on much data. Can I also ask, what the hell is up with this scale’s color scheme:
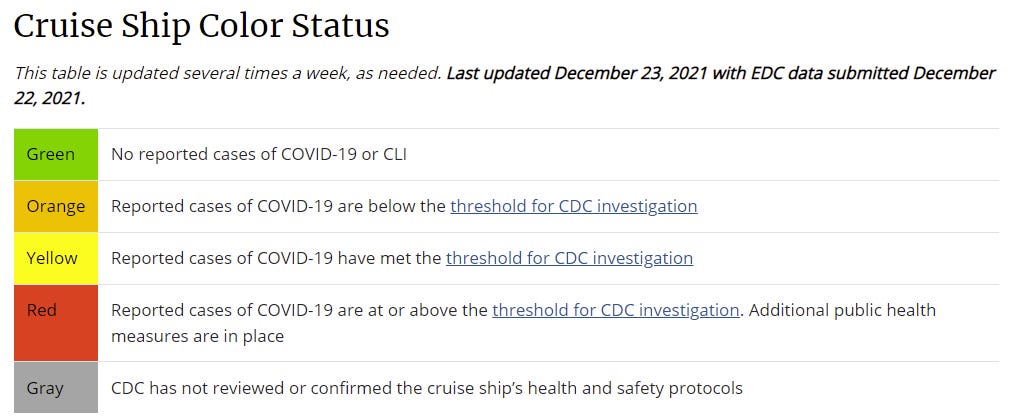
The majority are indeed in yellow, with some in green, and only a handful are orange. Having only a few Omicron cases isn’t a thing. I’d be curious to compare to past patterns, but it’s not obvious how to do that. Also, despite dozens of ships in yellow with ongoing investigations, zero ships currently are in red, meaning no one has ‘additional health measures in place.’
To what extent do you think the Chinese know this ‘disinfecting’ is the Goggles, and does nothing, but are doing it anyway? And to what extent do they actually think it matters? And to what extent is it a way to ensure people stay home?
Probability Updates
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 70% → 65%.
The South Korean study points again to very short generation times, but with wide error bars. If it’s on the lower end, then we’re not going to hit the 100% threshold here. Warning flag that I may be under-updating here.
Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 75% → 80%.
Chance that Omicron is vastly (75%+ in the same person) less virulent than Delta: 15% → 20%.
The data from London and elsewhere, and the general lack of bad news on such fronts, should make us more optimistic. Most cases being incidental is happening again.
Will the CDC label Omicron a variant of high consequence before 2022? 5% → 1.5%.
We’re out of time, and nothing happens this late in the year. Delisting unless it happens.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 25% → 25%.
No developments here, and time passing shouldn’t change things much.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 20% → 15%.
The longer things mostly hold up, the less likely this becomes. We’re getting closer to being in the clear.
Generation time (serial interval) of Omicron is 3.5 days or less: 75% → 85%
The South Korean study seems like strong evidence in favor of this.
I’m from Germany and want to respond to this:
I think the regulations were tightened because of the growth of Delta. The decline in cases is just for Delta. Omicron hasn’t taken over yet but because of the risk of it the lockdown is still in place.
I have been tracking Omicron numbers for a while now and even with a daily growth of ~30% (has been relatively stable both globally and in Germany) it can’t have reached a significant fraction of the population even assuming a high unknown percentage.
Yep, that seems like the right explanation. It’s coming, but you’ve stalled it for a bit.
Berlin’s numbers show about 20% Omicron for last week and about 3% for all of Germany. So at least in Berlin, it’s already there (and numbers should be >50% omicron with new year’s eve.)
In Hamburg, the numbers are also high. The same as London, New York, and all other dense connected traffic hubs. But even in Hamburg Omicron hasn’t taken over yet—though it can’t take much longer.
For reference, in neighboring Switzerland we did not stall with any significant lockdowns, and omicron is starting to take over only this week. Yesterday was the first time a clear uptick was visible in total case counts (delta + omicron), after a period of case counts being almost flat.
I know it’s unlikely, but if it was indeed omicron, its faster generation time also would make its numbers drop faster if they managed to move R under 1
Latest data from the RKI is 17.5% Omicron for the week ending on december 26, up from 3.1% the week before. Regional differences seem to be huge, between 1% in Sachsen and 65% in Bremen.
Overall numbers—still mostly Delta—are still declining and should turn upward again in 1 or 2 weeks.
That graph seems to be saying 9/1000 Londoners have COVID, not 9%
Hm, that would be really low. The Zoe Covid app right now estimates between 4.1% and 7.4% of symptomatic Covid for London burroughs.
I am confident the y-axis label is wrong and it’s 9%.
The guy who published the graph on Twitter admits he made a mistake and it’s actually 9/1000.
https://mobile.twitter.com/john_actuary/status/1474401836471918603
So there’s no source which says 10 percent have COVID, even if you personally think they do.
Yeah the thing is I was about to correct it based on that but 9/1000 makes no sense. Would be lower than other areas.
Turns out you were right: https://twitter.com/john_actuary/status/1474418553545756694
I’m not sure why. There’s 90,000 cases a day in the UK. That’s roughly 1 per thousand. If we merge cases from the last couple of weeks that’s closer to 9 in a thousand than 9 in a hundred.
Hello,
Firstly, I follow your CoViD posts with great interest, and would like to say thank you very much for the work you put into this project.
I wanted to direct you to the Colorado state CoViD data portal, which I only recently discovered. I saw that you’ve included Washington state data and thought it might help to have an easy visual reference to compare states/regions. It contains a fair amount of data the state collects on various aspects of the pandemic; healthcare impact, testing, cases, etc. Of note is the variant surveillance data; a week-by-week graphic for relative proportions of variants is available, and is very illustrative particularly of the spread of Omicron. The comparison to Delta is fairly stark; Omicron has approached fixation more than twice as fast as Delta in the state. The sequencing sampling methodology could lend itself to imprecision (only a small proportion of positives are sequenced), and much of the data provided upfront is aggregated over the entire course of the pandemic for some reason, but there may be something of value either on this page or the various resources provided therein:
https://covid19.colorado.gov/data
Once again, thank you for these posts, and I hope this will be of some use.
BBC reports today (i.e. after post was published) that 3 in 10 people who are in hospital with COVID in England were admitted for something else.
https://www.bbc.co.uk/news/uk-59814032
Thanks. Now all we need is a historical baseline...
Huh. Just like in Parasite.