Health officials look on in horror as individuals both vaccinated and unvaccinated, and state and local governments, realize life exists and people can choose to live it.
This is exactly what I was worried about back in December when I wrote We’re F***ed, It’s Over. The control system would react to the good news in time to set us up to get slammed by the new strains, and a lot of damage can get done before there is a readjustment. The baseline scenario from two months ago is playing out.
The good news, in addition to the positive test percentages continuing to drop for now, is that we have three approved vaccines rapidly scaling up and are well ahead of the vaccine schedule I anticipated, having fully recovered from last week’s dip, and it looks like the new strains are more infectious but not on the high end of the plausible range for that.
The J&J vaccine was approved this week, after a completely pointless three week delay during which no information was found and (for at least the first two-thirds of it) no distribution plan formed. Anything I put at 98%+ on a prediction website isn’t fully news, but the other 2% would have been quite terrible. Supply will initially be limited, but will expand rapidly, including with the help of Merck.
Meanwhile, now that we were provided a sufficiently urgent excuse that we were able to show that mRNA vaccines work, we’ve adopted them to create a vaccine for Malaria. Still very early but I consider this a favorite to end up working in some form within (regulatory burden) number of years. It’s plausible that the Covid-19 pandemic could end up net massively saving lives, and a lot of Effective Altruists (and anyone looking to actually help people) have some updating to do. It’s also worth saying that 409k people died of malaria in 2020 around the world, despite a lot of mitigation efforts, so can we please please please do some challenge trials and ramp up production in advance and otherwise give this the urgency it deserves? And speed up the approval process at least as much as we did for Covid? And fund the hell out of both testing this and doing research to create more mRNA vaccines? There’s also mRNA vaccines in the works for HIV, influenza and certain types of heart disease and cancer. These things having been around for a long time doesn’t make them not a crisis when we have the chance to fix them. And your periodic reminder that the same is true of health’s final boss, also known as aging.
Also, please note that I have been given the opportunity to offer Covid Micro-Grants; see the section below for details. If you can use $1k-$5k to complete a project to help with Covid-19, please don’t hesitate to apply.
Let’s run the numbers.
The Numbers
Predictions
Last week: 4.9% positive test rate and an average of 2,068 deaths.
Late prediction (Friday morning): 4.5% positive test rate and an average of 1,950 deaths (excluding the California bump on 2⁄25).
Result: 4.2% positive test rate and an average of 1,827 deaths after subtracting the California bump.
Great news. I’ve found it pays to be conservative in predicting changes, so when we get the full ‘baseline scenario’ style changes like this, I’m going to undershoot. This was essentially the good scenario, and it bodes well. Deaths continue to lag behind, despite increased vaccination effects for the elderly, in ways I don’t entirely understand. The theory that it’s lag can’t explain the bulk of it because it doesn’t match the past data.
Deaths
NOTE: Arkansas reported net negative deaths this week, which seems unlikely, so I set them to a plausible but low number (40) instead.
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Jan 7-Jan 13 | 6280 | 3963 | 7383 | 4752 | 22378 |
| Jan 14-Jan 20 | 5249 | 3386 | 7207 | 4370 | 20212 |
| Jan 21-Jan 27 | 6281 | 3217 | 8151 | 4222 | 21871 |
| Jan 28-Feb 3 | 5524 | 3078 | 8071 | 3410 | 20083 |
| Feb 4-Feb 10 | 4937 | 2687 | 7165 | 3429 | 18218 |
| Feb 11-Feb 17 | 3837 | 2221 | 5239 | 2700 | 13997 |
| Feb 18-Feb 24 | 3652 | 2433 | 4782 | 2427 | 13294 |
| Feb 25-Mar 3 | 3834 | 1669 | 5610 | 1958 | 13071 |
There is no plausible story where deaths in the south could be on the uptick for real, but the Arkansas adjustment goes the other way and there weren’t any other glaring mistakes. My assumption is that this is data lag after the storm and isn’t a real change, slash there’s a lot of noise in when deaths are measured in ways that still do not make sense to me but which have happened too many times to not acknowledge.
Positive Tests
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Jan 21-Jan 27 | 260,180 | 158,737 | 386,725 | 219,817 |
| Jan 28-Feb 3 | 191,804 | 122,259 | 352,018 | 174,569 |
| Feb 4-Feb 10 | 144,902 | 99,451 | 255,256 | 149,063 |
| Feb 11-Feb 17 | 97,894 | 73,713 | 185,765 | 125,773 |
| Feb 18-Feb 24 | 80,625 | 64,857 | 150,493 | 110,339 |
| Feb 25-Mar 3 | 66,151 | 58,295 | 151,253 | 115,426 |
Test counts bounced back this week and that’s likely accounting for the bumps up in raw positive test counts in the Northeast and South. The situation is still clearly improving. Doesn’t mean I would start lifting mask mandates.
Test Counts
NOTE: This table will not be in future editions unless I can find a new data source for it that’s reasonable to use. Suggestions for a new data source are great.
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| Jan 7-Jan 13 | 13,911,529 | 12.2% | 1,697,034 | 6.6% | 6.97% |
| Jan 14-Jan 20 | 14,005,720 | 9.7% | 1,721,440 | 5.9% | 7.39% |
| Jan 21-Jan 27 | 12,801,271 | 8.8% | 1,679,399 | 5.3% | 7.73% |
| Jan 28-Feb 3 | 12,257,123 | 7.7% | 1,557,550 | 4.6% | 8.02% |
| Feb 4-Feb 10 | 11,376,541 | 6.4% | 1,473,454 | 4.1% | 8.25% |
| Feb 11-Feb 17 | 10,404,504 | 5.2% | 1,552,555 | 3.5% | 8.41% |
| Feb 18-Feb 24 | 9,640,109 | 4.9% | 1,502,741 | 3.2% | 8.55% |
| Feb 25-Mar 3 | 10,610,092 | 4.2% | 1,701,829 | 3.1% | 8.69% |
The bounceback in test counts helps explain how positive test percentages fell so much week over week, and makes trends in New York look troubling. I’m going to be in the city this coming week, and it might be that I got in exactly in time given I’m not yet vaccinated.
Vaccinations
Our progress here suddenly looks great. I expected a surge to happen in March and am pleasantly surprised to see it happen this large and this quickly. The one concern is if a bunch of this is catch-up efforts after the snowstorms cleared, in which case we might effectively be back on our old pace for a few more weeks.
The future numbers are even more promising, if you can wait a few months:
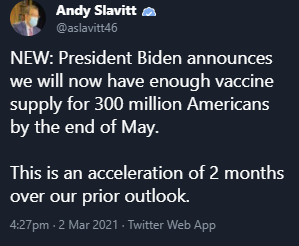
I’m quite happy about this of course, and do expect the vaccines to arrive, but in an important sense it’s important to realize this is literally Fake News. What’s fake is the claim that this is news, that something has changed. Nothing changed. Biden has been pursuing a hyper-aggressive policy of under-promise and over-deliver to the point of absurdity, in order to claim maximum credit. This is the natural result. I do understand the motivation, but in addition to the continuing damage to his credibility and government credibility in general (which is bad for vaccines in particular, but in general represents a truth-tracking update) it is of course highly unhelpful. If you want people to hold the line, telling them the end is in sight is exactly what you should be doing. Especially if it’s true.
The question is whether we can count on this pattern to continue. I don’t mean that in a judgemental way, I mean that in a truth seeking way. If we can assume that what is said is designed to make the end result look as impressive as possible, then we can properly evaluate the claims coming from the new administration. We’d get to have Pravda which always lies (in the same directions), instead of the New York Times which keeps you guessing by sometimes telling the truth. It would be especially nice if this pattern extends beyond the pandemic. Presumably at some point there will be a time to claim to have delivered the goods, which complicates matters.
Could it be? Vaccinating people overnight?
We finally are going to vaccinate at night, it seems, in order to make it clear who is getting which vaccine. Or, alternatively, we can think of this as offering the rent-controlled good-but-hard-to-get thing during the day (Moderna/Pfizer vaccine at a time you want to be awake) versus the market rent good-enough thing at night (J&J vaccine, which you bid on by willing to make a trip in the middle of the night at increasingly terrible hours). It’s a really bizarre way to do a little bit of an obviously correct thing, but at this point we’ll take whatever we can get.
Meanwhile, in North Carolina they have open vaccinations except for those who refuse to lie to government officials, who go to the back of the line:
How much is vaccine capacity worth, and how much are we underinvesting in it even now? About this much.
How good is our vaccine prioritization? About this good:
How much are we gonna have how fast? Hopefully this much, and hopefully faster:
Faster wouldn’t actually surprise me, since we have an authority systematically under promising.
Europe
It is Italy’s turn to worry as cases trend upwards. Mostly it seems like Europe is doing what it takes to stabilize things while it suffers several months of extra pain thanks to their collective decision to be penny pinchers with regard to vaccines. That decision seems like the essence of the European project at this point, emphasizing things seeming fair and polite and making sure everything abides by all the rules and regulations, whether or not that is compatible with life. One must not underestimate the value of keeping the peace, but these trends likely keep accelerating, and I doubt it ends well.
Farewell, Covid Tracking Project
On March 7, the Covid Tracking Project will stop collecting data. There are many other data sources out there, but I still don’t have one I’m fully happy with. I primarily want easy access in table form of the number of tests, positive tests, hospitalizations and deaths, on a daily basis, including a full history. This needs to be available for the nation and if at all possible for individual states; more granularity beyond that is a bonus, as is any additional data.
John Hopkins has been suggested as an alternative data source. The data itself seems excellent, but like most places they seem obsessed with giving it to us in graph form rather than table form, which is useful at a glance but super frustrating when I’m trying to create spreadsheets and my own graphs and charts. Also, they list their data source as… the Covid Tracking Project. So they have the same problem I do, and we’ll see if they still have good data next week.
Anyway, once again opening the floor for any suggestions.
The wikipedia data on deaths and positive tests is great, but as far as I can tell it doesn’t include the number of tests, so it doesn’t tell me the denominator (the total number of tests).
Announcing Covid Microgrants
Thanks to a donor who wished to remain anonymous, I am able to offer Covid microgrants. These will be grants of $1000 to $5000 each, for those who have a Covid project which they could finish given this small amount of additional funding. If you’re interested, fill out this Google form. Applications close on 3/12/21, and decisions will be quick and based only on my own judgment. I am very curious to see the quantity and quality of applications that come in, and if things go well this could happen again. Please don’t hesitate to apply, or to encourage others to apply.
Insert Mission Accomplished Banner
This kind of thing continues to happen, here’s where we were on February 25:
And here’s where they were three days later:
Then the next day, in Texas:
The English Strain
Why do people keep making this mistake over and over again and I don’t mean Greg Abbott:
This is showing up in the case numbers! It’s showing up as a 20%-30% increase in cases!
Very few people who got infected by a B.1.1.7 strain would have otherwise gotten infected by the old strain during this same time period. Very few people who got infected by a B.1.1.7 strain would have been infected if the initial people to have B.1.1.7 had the old strain instead, because its additional infectiousness has grown its share of infections by several orders of magnitude.
Thus, if you have 80 infections with the old strain and 20 with the new, and no one’s had time to change their behaviors in response yet, this is showing up in the case numbers as about 20 new cases. It’s at least 19.
That’s how to track the impact of the new strain: All cases of the new strain should be considered ‘extra’ cases due to the new strain, until there’s enough time that the control system has adjusted behavior to account for the new infections. Period.
The switch to primarily B.1.1.7 infections seems to be poised to happen in early to mid March, which is later than I feared but clearly in the middle of the expected range.
Johnson, Johnson & Merck
In excellent news, pharmaceutical giant Merck, whose Covid-19 vaccine candidate didn’t work out, is going to help make the Johnson & Johnson vaccine (WaPo). Wonderful, and exactly how it should go. There’s available capacity (not necessarily fully free capacity, but this is a priority), everyone makes a deal, profits, looks good and does good doing it, presto.
That’s great news, and can make us even more confident we will have enough vaccine supply in the medium term, and more confident we’ll be able to help vaccinate the whole world soon after.
What this highlights is how bad the delay in approval of J&J’s vaccine was. J&J was already making doses using its own capacity, so there was a story one could tell that while this delayed some doses being delivered by a few weeks, it didn’t destroy capacity or change the long term trajectory. If days after approval, they’re finally getting to a deal to get Merck to step up, it seems very likely this deal had to wait on approval, so this pushed back half or more of J&J’s long term capacity by three weeks. That’s going to kill a lot of people.
Stockholm Syndrome
This is quite the graph, showing weekly Covid levels in the Stockholm wastewater:
(I assume Week 1 here means 2021 Jan 1-7, and so on.)
There is clearly a lot of measurement error here. There aren’t worlds in which week 4’s levels should be more than double both week 3 and week 5’s levels, nor does the jump from 42 to 43 or 34 to 35 make any sense. The last measurement is plausibly a pure data error. My best guess is that the sample isn’t effectively being taken from distinct enough locations and is effectively measuring something too local, and caught a local outbreak? Regardless of the right explanation, there’s still something being measured here, and this is the definition of off the charts. Seems worth noticing.
Noticing this, I checked in with Boston wastewater as well:
There was an upward move, but things seem to have come back and now are below the previous low point this year, so it seems like things are indeed continuing to improve. It does provide an additional suggestion that there was some sort of brief mini-surge corresponding to the uptick in numbers, but I have actual zero idea what could have caused that at that time.
Vaccines Still Work
Vaccines still work, Pfizer single-dose preventing infection edition.
Vaccines still work, Moderna single-dose preventing infection edition. More lowballing.
Vaccines still work, AstraZeneca and Pfizer single-dose edition (paper).
Vaccines still work, take essentially any vaccine you can get edition (MR). Chinese vaccine is the only plausible exception.
Vaccines still work, second doses still wasteful and J&J approval exposes this once again edition (MR).
Vaccines still work, but keep not getting approved, so here’s the rich Germans will fly to Russia, get vaccinated and leave without ever entering the country edition.
Vaccines still work, they all are awesome, but some are better than others and while you should mostly take whatever is available, you should care a nonzero amount about getting the best one you can edition, a Jason Furman Twitter thread.
Vaccines still work, we fully knew this back in July and everyone who stalled things further should be judged accordingly edition.
In Other News
We can all agree Andrew Cuomo is the worst, it seems, due to claims of sexual harassment. We were going to let the causing of and then covering up of thousands of deaths slide – I mean what politician hasn’t done that sort of thing this past year – but we have a zero tolerance policy for sexual harassment that reaches a threshold level of social media prominence. This calls for an independent investigation immediately. I’d summarize my reaction to all this as: I’m not saying Al Capone wasn’t guilty of tax evasion, and also I’m shocked, shocked to find gambling in this establishment.
It appears Operation Warp Speed had to be funded by raiding other sources because Congress couldn’t be bothered to fund it. As MR points out, this is a scandal because it was necessary, rather than because it was done. It’s scary, because it implies that under a different administration Operation Warp Speed could easily have not happened at all.
Catholic Church tells members to avoid J&J vaccine if they can, over concerns about abortion, despite Pope explicilty saying those concerns don’t apply. Divine authority, you had one job!
Another reason you might want to pay money for the things you want:
Shed a tear for maybe it would also have been even more helpful to make the vaccine profitable back when it could have helped increase supply but also take whatever we can get, wherever we can get it.
Doctor Fauci’s defense against First Doses First is a combination of pure FUD and… that it would be a messaging problem?
Also that we’ve already missed the window where this would have helped much, thanks to people like him dragging their feet on this and continuing to drag their feet, so no point in worrying about it now, might as well acknowledge that the foot dragging worked:
At least the ‘this would further blow our credibility’ argument is honest and has content. It’s true that reversing these policies, when the need for first doses first is getting less rather than more urgent, would make those involved look like lying liars and/or bumbling idiots, who mostly aren’t optimizing for outcomes, and for various reasons they’d prefer a less accurate perspective to retain its popularity.
Fauci’s new position is that ‘there are risks to both approaches’ and to continue to use variations on ‘no evidence’ and to emphasize that the second dose offers an individual additional protection, as if that was in any way in dispute. The concept of a cost/benefit analysis, or the idea that one might shut up and multiply, let alone form a detailed model full of gears, is clearly not within his range.
At least Canada is increasingly doing First Doses First. Their statement is bold and excellent.
Zeynep post and open thread on pandemic lessons for the future.
Zeynep article in The Atlantic about how our public health messaging has been a disaster.
Post is excellent, and does a great job driving home the central things that went massively wrong with public health messaging. My only quibble is that harms from terrible regulation are treated as beyond scope and not discussed, which is reasonable in context but also feels like ignoring the elephant. Also, if you’ve been following events via my posts, Zeynep’s post is largely a case of You Should Know This Already.
In particular, Zeynep points to five key mistakes: Fear of risk compensation, telling people to use rules instead of mechanisms or intuitions, scolding and shaming especially for outdoor activities (which is a lot of why parks/beaches were closed while indoor gyms were permitted in many places), failure to support or give people tools for harm reduction while making impossible asks (e.g. no socializing for a year), and sitting on the line of ‘no evidence’ or ‘no clear evidence’ over and over and over again.
And yes, she points out, still doing it:
We did it with masks, with transmission methods and modes of prevention, and now again and also with vaccines.
That’s all an excellent summary of the biggest failures, but I am not convinced it is fair to call them ‘mistakes.’
All of this also isn’t new, this isn’t Covid but seems highly on point (OP has lots more and is great):
Then of course because don’t be absurd and I’d be boggled to find a different answer:
Canada authorizes AstraZeneca.
Dr. Fauci graciously says it’s all right for two vaccinated individuals to have dinner together, citing “common sense” and that the risk is “extremely small.” The implication that all people involved must be vaccinated is clear, so this is a retreat from one insane position to a slightly less insane position.
Update on the White House supercluster of infections, which happened exactly the way one would expect, so no real need to click.
We shouldn’t expect anything less. CDC guidelines for citizen behavior have always been at best aspirational (you could also use the word ‘crazy’) and mostly ignored. This never seemed wise to me, since once one realizes one is not going to do what the authority demands, one often ends up doing little or nothing.
The danger is that we may have entered a new mode where people might actually listen to the CDC guidelines and make serious attempts to get people to follow them, perhaps indefinitely. “Infectious disease specialists” are like any other ‘specialist’, and think everyone should pay dearly to solve the particular problems they think about all day regardless of whether the cost/benefit analysis would make any sense if someone ever did one. If you didn’t ignore most such ‘specialists’ you’d do nothing else all day and feel bad about falling short anyway.
Is Biden ‘following the science’ (MR) as promised? Tyler Cowen says no and presents his case. The administration allowed the CDC to issue nonsensical guidance that is similar to its usual nonsensical guidance except it’s often going to actually get followed, which is preventing the reopening of many child prisons. AstraZeneca and other vaccines remain unapproved and J&J took three weeks to approve. There is no new head of the FDA and no talk of FDA reforms of any kind. He doesn’t mention vaccine prioritization, which was also massively botched by every metric one might plausibly care about. Post also mentions some non-Covid decisions
I think Cowen’s interpretation here is wrong, and Biden is indeed Following The Science exactly the way he promised. He’s not following the science, in the sense in which science is the collective methods by which people know things, via such actions as doing experiments, gathering data, modeling the world and figuring out what causes and actions might have what effects so as to choose better causes and get better effects. He’s (Following Science
Not Covid, but Eliezer Yudkowsky science fiction ethos recommendations seem worth sharing.
Administrative Note
This week I will be in New York City. This will be awesome, and I look forward to my permanent return soon. It also means I will have limited resources and time in which to work on the post next week. It may be relatively abridged, and there is some chance it will come out on Friday instead.
You need to change the sharing settings on the application form for microgrants. Also, great post as always, you’re my hero :D
There are gaps in the reporting on Operation Warp Speed funding, because apparently a bunch of the money that Congress did allocate for vaccines hasn’t been spent yet. I don’t understand why the White House spent other money but not that money.
What update is this supposed to cause for Effective Altruists? We already knew that policy around all sorts of global health (and other) issues is very far from optimal, but there’s nothing we can do about that. Even a global pandemic wasn’t enough to get authorities to treat trials and approvals with appropriate urgency and consideration of the costs of inaction, so what hope would a tiny number of advocates have? We can fantasize all day about what we’d do if we ran the world, but back in reality policy change is intractable and donating to incrementally-scalable interventions like bednets remains the best most of us can personally do. Or am I misunderstanding what you meant here?
(Note also that malaria vaccine human challenge trials were already a thing; Effective Altruist John Beshir participated as a subject in one in 2019.)
I’m saying you should consider funding more basic research like mRNA vaccines and less bednets. Or setting up medical cruise ships for challenge trials in international waters. Or focusing on epistemics or even policy.
Also, if the pandemic wasn’t obviously net bad that raises a lot of questions...
- Is there any reason to think research that could lead to malaria vaccines is funding-constrained? There doesn’t seem to be any shortage of in-mice studies, and in light of Eroom’s Law the returns on marginal biomedical research investment seem low.
- Malaria is preventable and curable with existing drugs, so vaccines for it only make sense if their cost (including required research) works out lower than preventing it in other ways, which means some strategies that made sense for something like Covid won’t make sense here.
- That’s not how international waters works, you’re still subject to the jurisdiction of the flag country and if they’re okay with your trial you could do it more cheaply on land there.
- If you attempt an end-run of the developed-country regulators with your trial they will just refuse to approve anything based on your trial data, which is why pharma companies don’t jurisdiction-shop much at present.
- That said developed country regulators do in fact approve challenge trials for malaria vaccines (as I noted) and vaccines for other curable diseases. Regulatory & IRB frameworks no doubt still add a bunch of overhead but this does further bound the potential benefits of attempting to work outside them.
- I don’t know what “focusing on epistemics” could possibly entail in terms of concrete interventions. Trying to develop prediction markets I suppose? I have updated away from the usefulness of those based on their performances over the past past year though, and it seems like they are more constrained by policy than by lack of marginal funding (at retail donor levels).
- Policy change is still intractable.
- In general there are lots of margins on which the world might be improved, but the vast majority of them are not plausibly bottlenecked on resources that I or most EAs I know personally control. Learning about a few more such margins is not a significant update. I focus on bednets not because I think it’s unusually much more important than other world-improving margins, nor because I think it will be a margin where unusually much improvement happens in coming years, but because it’s a rare case of a margin where I think decisions I can make personally (about what to do with my disposable income dollars) are likely to have a nontrivial impact.
Seconding Eliezer’s recommendation for the Young Wizards series; I’d call them the most important fiction I’ve read.
And cheap ebooks are available direct from the author, eg https://ebooks.direct/products/the-i-want-everything-youve-got-package (and the Tale of the Five series is probably also of interest to anyone who can spell “polycule”).
Note that if you are in the UK, that link will not work. (For me, exactly what happens depends on what browser I’m using, but a typical experience is that it displays the bundle you intended, and then after about a second it switches to displaying a grid showing all their products, and then after about 1⁄3 of a second those all disappear, leaving me on a shopping page where I cannot in fact either view or buy anything.)
The reason, looking at their blog, appears to be that their response to the extra bureaucracy they face post-Brexit is to give up on selling to the UK, so they just filter out their entire product range if they detect that you’re in the UK. (You’d have thought it would be easy for them to put up a little notice saying why, so it doesn’t look like a bug, but no matter.)
The intended workaround for people in the UK is a thing that points you at places where you can buy their books (presumably at higher prices and with DRM) from Amazon etc., but that is currently unavailable and “will become available during the week of January 18-22, 2021”. I suppose it’s appropriate for SF&F authors to sell their books only to people capable of time travel.
Zvi—if you’re taking requests for the next update—would like reviews of the data showing J&J is better at the new variants (which ones and to what do extent and how certain are we)?
Just saw this now but if you link me to the info I’ll put in the queue for next week.
I don’t entirely understand the arguments myself, but it goes something like what MarketWatch said here:
“Experts are quick to point out that the clinical trials were conducted at different times — Pfizer and Moderna conducted their trials before several mutated variants had been reported, whereas Johnson & Johnson’s trials were conducted after that. Consequently, Johnson & Johnson has clinical-trial data to show its vaccine can work effectively against variants first reported in the U.K., South Africa and Brazil.”
https://www.marketwatch.com/story/the-backlash-against-johnson-johnsons-covid-19-vaccine-is-real-and-riskyheres-exactly-how-to-make-its-rollout-a-success-11615407137
They link to this ABC news page:
https://abcnews.go.com/Politics/single-dose-johnson-johnson-vaccine-effective-variants-data/story?id=76084549
That actually says it’s least effective against the South African variant.… so… there’s that.
I originally heard about it from my wife who heard about it from Sanjay Gupta’s podcast who said there was a study showing this, but I couldn’t find whatever Sanjay was talking about.
You can extract numbers from a graph if you have to
https://www.researchgate.net/post/What_is_the_best_free_software_converting_a_scanned_graph_plot_to_a_digital_plot_x_y_data
This is pretty awesome
Do we have numbers for how effective different vaccines are at stopping transmission of the virus? I looked through some of your old posts but couldn’t find numbers. Trying to figure out how much to discount the risk from getting together with some vaccinated friends.
Someone suggested to me recently that, against all appearances and expectations, the Trump Administration not buying enough mRNA vaccine for everyone right off the bat was actually the right call. We knew other vaccines were on the way which had way less exacting distribution conditions and/or were single-dose.
I suspect that proposition is Off in some important way, like the doses weren’t enough even to hold out for a switch out, and am curious what thoughts you all have about it.
It is off because if buying 100x what we need speeds up our vaccinations by one week we still got a fantastic deal, so you buy way way way too much of everything then donate or sell the rest to vaccinate the world be a hero and shut off or slow mutations and save lives.
We should have almost literally spared no expense.
It’s wrong because the first dose of the mRNA vaccine is approximately as good as the J&J vaccine. Give or take, “no evidence” blah blah blah. (what I am referring to is there is no gold standard RCT head to head comparing this exact scenario so we have ‘no evidence’ as to what will happen, we can only eyeball a graph and say, ‘well immunity seems to keep rising with the mRNA over time, and at 10 days it is about 50%, so it’s probably about 66% like the J&J vaccine at 30 days’. Similarly, we don’t actually know the J&J vaccine is any worse, there is “no evidence”, because it got tested with a different RCT, which means different people and possibly different strains of covid around. So there is a chance it has the same effectiveness as the mRNA vaccines but probably not)
Second, as you may have heard, the “exacting distribution conditions” were also overblown and it turns out a regular freezer is good enough, at least for a week, which is sufficient to distribute the doses.
Hmm....
Aha!
*
The “Vaccines still work” section is great
*
I guess this wasn’t intentional, but the comedic effect is fantastic:
*
At the current 6.36m rate of global vaccination per day, it will take 1250 days to fully vaccinate the world. currently the US accounts for a third of these daily vaccines. i hope this rate will continue to increase even after rich countries finish vaccinating their own populace.
At some point in the near future this rate will become unsustainable. Because vaccine hesitant and vaccine avoiders are a significant minority everywhere.
Near the end of the linked malaria article, it says:
So it sounds like maybe they are in act doing human challenge trials.
I remain extremely angry at the lack of clinical trials for indomethacin as an outpatient treatment.
Quick explanation of the weeks. It’s not the first time you mention that.
The rest of the world uses this method of counting weeks: https://en.wikipedia.org/wiki/ISO_week_date.
Week 1 is the first week (starting on Monday) with the majority of its days in January. This year started on a Friday, so we only had 3 days in Jan in the week containing New Year. As a result, we ended up with 2020 having 53 weeks.
So, on the graph, Week 53 is Dec 28 to Jan 3, while Week 1 is Jan 4 to Jan 10. We’re currently in Week 10.
I have wanted to look at the source code from rt.live for awhile. I’m not sure where they were getting their state by state data from. That might be a place to start? https://rt.live/
Also curious as to where https://covidly.com/ gets their data.
Any good links on this? My family took the chinese vaccine, and I would need to wait an extra month if I wanted pfizer.
No, this is on the basis of not trusting any claims from chinese scientists or studies because track record. So my heuristic is to watch what they do. If you can confirm that the top party officials got it, go for it. Otherwise, avoid.
Re the English strain, do you (still) think its dominating new cases by mid-March will lead to a huge increase in cases/deaths nationwide, or will vaccination prevent that?
The CDC’s latest ensemble forecast doesn’t predict an increase in deaths, though it only goes out to the end of March:
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/forecasting-us.html#anchor_1587397564229
I think it’s not clear which way it will go, depends on a bunch of unknown variables and where they land. The toy model can be tinkered with. But if it’s actually more deadly too then yes deaths almost have to rise before falling.
It now seems it’s about 60% more deadly:
https://www.bmj.com/content/372/bmj.n579
Ah I see you discuss this in your latest post, just posted.
If you’re willing to write a data extraction script, and John Hopkins continues updating from a new source (that doesn’t otherwise publish raw data), you can find the numbers on the embedded sub-pages:
https://coronavirus.jhu.edu/embed/testing/state-data/testing_per_state_New_York.html