Scott Alexander reviewed his Covid-19 predictions, and I did my analysis as well.
It was a quiet week, with no big news on the Covid front. There was new vaccine data, same as the old vaccine data – once again, vaccines still work. Once again, there is no rush to approve them or even plan for their distribution once approved. Once again, case numbers and positive test percentages declined, but with the worry that the English Strain will soon reverse this, especially as the extent of the drop was disappointing. The death numbers ended up barely budging after creeping back up later in the week, presumably due to reporting time shifts, but that doesn’t make it good or non-worrisome news.
This will be a relatively short update, and if you want to, you can safely skip it.
If anyone knows a good replacement for the Covid Tracking Project please let me know. Next week will be the last week before they shut down new data collection, and I don’t like any of the options I know about to replace them.
Let’s run the numbers.
The Numbers
Predictions
Last week: 5.2% positive test rate on 10.4 million tests, and an average of 2,089 deaths.
Prediction: 4.6% positive test rate and an average of 1,800 deaths.
Result: 4.9% positive test rate and an average of 2,068 deaths.
Late prediction (Friday morning): 4.5% positive test rate and an average of 1,950 deaths (excluding the California bump on 2⁄25).
Both results are highly disappointing. The positive test rate slowing its drop was eventually going to happen due to the new strain and the control system, so while it’s disappointing it doesn’t feel like a mystery. Deaths not dropping requires an explanation. There’s no question that over the past month and a half we’ve seen steady declines in infections, and conditions are otherwise at least not getting worse. How could the death count be holding steady?
One hypothesis is that weather messed with the reporting, but Texas deaths went down and the patterns generally do not match. Virginia saw a giant jump in the death rate and I’ve adjusted them down by 475 deaths to account for that, which seem to be holiday-related catchup even though it seems super late for that. Nothing else stood out in the charts. As per my rules, since the Virginia adjustment improves my accuracy and there’s a non-zero amount of ambiguity, I’m not including it in the results section. If included, that would move us to 2,001 deaths per day, which still feels too high.
Added Friday 9am: I realized this morning I hadn’t made a prediction, so I’m making one now, after seeing Thursday’s results that include a high death count (3138, 800 of which are a backlog from California), and a lot of tests (1.8mm) with only a 4.1% positive rate. I expect some continued improvement for now, but there are signs that improvement is slowing dramatically.
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Dec 31-Jan 6 | 4553 | 4127 | 5019 | 4162 |
| Jan 7-Jan 13 | 6280 | 3963 | 7383 | 4752 |
| Jan 14-Jan 20 | 5249 | 3386 | 7207 | 4370 |
| Jan 21-Jan 27 | 6281 | 3217 | 8151 | 4222 |
| Jan 28-Feb 3 | 5524 | 3078 | 8071 | 3410 |
| Feb 4-Feb 10 | 4937 | 2687 | 7165 | 3429 |
| Feb 11-Feb 17 | 3837 | 2221 | 5239 | 2700 |
| Feb 18-Feb 24 | 3652 | 2433 | 4782 | 2427 |
Using the Wikipedia numbers we do see continued declines in death rates, but still highly disappointing ones. The English Strain might be substantially more deadly, but it’s too early for that to account for this. It’s definitely odd and I not only see no explanations and lack a good one to offer, I don’t see anyone noticing that it is odd.
Positive Tests
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Jan 14-Jan 20 | 360,874 | 185,412 | 452,092 | 250,439 |
| Jan 21-Jan 27 | 260,180 | 158,737 | 386,725 | 219,817 |
| Jan 28-Feb 3 | 191,804 | 122,259 | 352,018 | 174,569 |
| Feb 4-Feb 10 | 144,902 | 99,451 | 255,256 | 149,063 |
| Feb 11-Feb 17 | 97,894 | 73,713 | 185,765 | 125,773 |
| Feb 18-Feb 24 | 80,625 | 64,857 | 150,493 | 110,339 |
Continued improvement, but slower than one would like especially given the continued drop in testing. We may not have much more time to see declines before counts start increasing again.
Test Counts
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| Jan 7-Jan 13 | 13,911,529 | 12.2% | 1,697,034 | 6.6% | 6.97% |
| Jan 14-Jan 20 | 14,005,720 | 9.7% | 1,721,440 | 5.9% | 7.39% |
| Jan 21-Jan 27 | 12,801,271 | 8.8% | 1,679,399 | 5.3% | 7.73% |
| Jan 28-Feb 3 | 12,257,123 | 7.7% | 1,557,550 | 4.6% | 8.02% |
| Feb 4-Feb 10 | 11,376,541 | 6.4% | 1,473,454 | 4.1% | 8.25% |
| Feb 11-Feb 17 | 10,404,504 | 5.2% | 1,552,555 | 3.5% | 8.41% |
| Feb 18-Feb 24 | 9,640,109 | 4.9% | 1,502,741 | 3.2% | 8.55% |
New York continues to test robustly, but many other places are not following suit. This continues to mean that the positive test rate is dropping slower than the true rate of new infections, but it’s also worrisome that we are getting out of the habit of testing people. This is nowhere near enough testing.
Vaccinations
It is hugely disheartening to see our weekly rate decline from 1.61 million per day last week to 1.3 million per day now, with no signs yet of a full recovery let alone getting back on our previously accelerating path. I do hope that will happen soon, and slow progress is still progress in the meantime, but it’s all scary.
How are we doing vaccinating nursing homes? About this well:
A line for only those not in nursing homes would make this contrast even more stark. We botched this job, but even with that botching it was hugely impactful.
Pfizer and Moderna claim to have solved their bottlenecks and pledge massive boost to US supply (WaPo). They are promising 140 million doses over the next 5 weeks, more than double the recent pace of vaccinations.
If we do get to that pace, we will be back on track to be able to give vaccine shots to everyone who actively seeks them out by the end of April, even if we don’t get our act together on half doses or first doses first or get any help from Johnson & Johnson or our other known safe and effective vaccine options.
On the first doses first front, yet another group of experts is out in favor of this obviously correct approach:
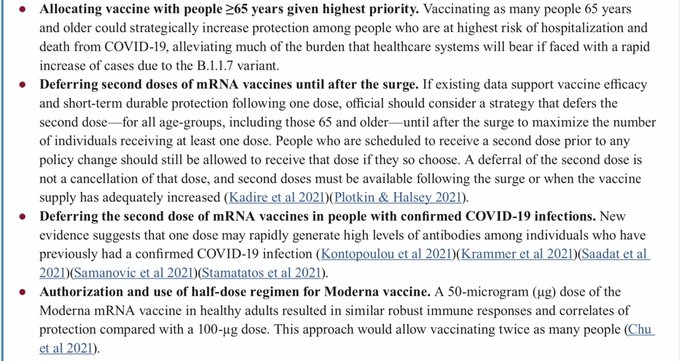
What I find most interesting is the explanation that this is motivated by the English strain:
The English Strain didn’t change the right answer. Instead, it puts additional pressure on the answer to be correct, giving a sufficiently short time-horizon problem slash scary downside scenario to allow ‘experts’ to come out in favor of the better answer over the worse answer. Whatever prevents the most infection, hospitalization and death is the right answer either way, and that’s far and away first doses first.
What would a country actually using its vaccine doses look like? I’m guessing something like this:
At a minimum, it would look like this:
Europe
You can see Europe’s situation mostly holding steady here, and you can see America’s death rate having climbed back up in the last few days (even adjusting for Virginia). It’s definitely troublesome.
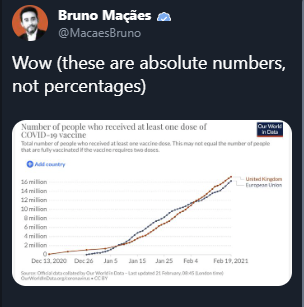
UK vs. EU vaccine efforts, looks like a tie, oh wait:
Covid Machine Learning Project
Yet another place to see the drop in vaccinations recently, especially in first doses. Other than that, the lines continue to move in the same directions previously expected. He now has us up to 28.1% ever infected as of February 11, and 13.8% having at least one vaccine dose as of today.
The English Strain
Some hard data from NYC (full report):
This seems like very good news given our priors. If we are only up to 6.2% now versus 2.7% for all of January, then the variant isn’t on pace to take over for another few months. That would be enough time to offset the increased infectiousness via additional vaccinations.
Alas, data elsewhere in the country is not as promising. This is another data source, this one covering sequencing in the United States, showing us in the 15-20% range.
Kai’s latest update on Denmark, where new strain is now 57% of cases, and cases are rising despite the lockdown.
Some hard data from a variety of countries, this website seems great. Doesn’t paste well, so click on the link. In the USA it has the English strain up into the low double digits, which is closer to my overall prior and still importantly better than I’d feared.
A Youyang Gu thread looks at various possible scenarios, and noting that new variant takeover need not mean we get a gigantic wave.
The South African Strain
A well-deserved break from insanity is now official:
A thread goes over the key passages:
This looks like an eminently sensible system. One age group, one week to assess safety, effectiveness judged straightforwardly based on immunogenicity.
Also good is that South African cases have fallen dramatically down, which should lower our worries about this strain on multiple levels.
Also, Moderna is testing an updated vaccine designed for the South African variant. It’s good news to confirm this but it was so inevitable it almost isn’t news.
Johnson & Johnson
The FDA has announced that the Johnson & Johnson vaccine meets the requirements for emergency authorization. You might think this would mean it is now authorized for emergency use. You would be wrong. You can’t rush meetings.
You might think that would mean we have a plan for what to do when it is so authorized. You’d be wrong again. Remember when Biden complained that Trump didn’t have a plan?
WTF, indeed. Taking three weeks to approve the vaccine is bad enough, but I can sort of understand it. Not using that time to make a distribution plan (this should not even be necessary, the plan should already have existed long ago) is a whole different level of sabotage. Rumors of the new administration’s ability to administrate seem greatly exaggerated.
Vaccines Still Work
Latest confirmation that vaccines work, in this case one shot of AstraZeneca:
Meanwhile, America continues to sit on a massive unused supply of AstraZeneca doses. What is the right way to describe that FDA decision?
Chinese data reports their vaccine also works, with effectiveness levels similar to Johnson & Johnson. Note that I say their data reports, rather than that it is true. Watch who gets vaccinated.
People continue to treat confirmation that vaccines work as news. It is not news.
We know vaccines work. They are highly (but not fully) effective in preventing infection and the spread of disease. They are even more effective at preventing severe disease, hospitalization and death.
That doesn’t mean that getting the exact numbers right isn’t valuable. Getting it right is valuable.
But those who imply, or outright say, that this is the ‘first information’ we have or that it is the ‘first evidence’ or anything like that, shame, shame, shame, shame on you.
No shame here, only facts (some shame further down thread but let’s ignore that):
If anything I find this a little disappointing, as I was very much enjoying the straight 100%s. Still, don’t get me wrong, I’ll take it.
Then there are those that are still going with the ‘no evidence’ line somehow. Note the date.
Shame.
This leads us to your periodic reminder:
There are no CDC guidelines for what vaccinated people should do.
After what happened with the schools, I’m not optimistic about what those CDC guidelines are going to say. The good news is that people are not schools, and can more easily hit ignore.
What the hell, Dr. Fauci? You were supposed to be lying to get better outcomes…
Who cares if you’re vaccinated, same energy, f*** everything, we’re doing five blades.
What happens when your messaging is all about how vaccination priority is the most important thing and also how vaccines can’t be relied upon in any way: Many NBA players reluctant to promote vaccine, largely out of concern that getting the vaccine too soon would look bad, but also because many of them don’t trust the vaccine.
You also get reactions like this:
I am not claiming that ‘tell the truth’ is always the correct simulacra-level-2 play, but blatantly lying to the public to their faces, in order to scare them and warp their perceptions of physical reality to get them to do what you want, is a strategy that keeps getting tried by elites and media, and keeps blowing up in their faces.
Good news, in the UK you’d at least be able to travel:
The continued FUD around whether previous infection protects people continues to be insane, as is forcing those already infected to compete for limited vaccine supply. The people I know (or secondhand know) who got Covid mostly then got the vaccine anyway, and worries about being punished for not having done so are a lot of the reason for that. Great strategy.
When is it time to go back to normal? Youyang Gu offers one perspective, the graph seems optimistic but the curve seems mostly reasonable:
There will come a day when there is once again a pivot, from everyone must take precautions to everyone must do their part to restart the economy. It probably won’t be as bad as the UK’s payments for dining in and only dining in during a pandemic that paid more if you had a larger group. It should still be expected to be perverse, because the system selects for perversity.
People like Dr. Fauci will instantly transform from ‘even fully vaccinated you can’t see a movie’ to ‘it’s important for our economy and mental health for us to get back to our regular lives.’
And then, if necessary, they’ll transform back, as many times as necessary.
This week we saw one of the first signs. Cuomo is proposing a $5,000 reopening tax credit per employee for restaurants (max 10 per restaurant).
So, let me get this straight. Restaurants are in danger of closing, so we’ll hold off on paying them for a year, then pay them money if and only if they reopen, exactly at the moment they’re not in as much danger of permanently closing. So if you managed to survive without payments, congratulations, you deserve a reward check? But only if you open now? It’s as if we wanted to transfer funds to restaurants, but held off until now because doing it earlier would have been helpful. If we do it now, it’s in the name of Economic Recovery, so giving preferred interests cash is now fine.
In Other News
From The Onion, on Cuomo, but don’t tell me you think it didn’t happen.
Meanwhile, in Florida, this is how the news covers…
…prioritizing the most vulnerable citizens (the elderly) for vaccination.
They also continue to use outdoor events as their go-to blame totems and cite them as superspreader events, despite this consistently proving not to be the case. Our continued closing of outdoor spaces and preventing outdoor activity is actively counterproductive on every level, so doubtless it will continue until this is fully over.
Thread by Youyang Gu of the Machine Learning Project, on whether in-person instruction at universities impacted Covid-19 rates. He concludes that, while there was a short-term bump in cases when classes began, there was no clear long-term rise in cases.
Marginal Revolution reminds us that “medical ethics” has no interest in benefiting humans or making the world a better place, is instead actively working to make the world a worse place and ensuring that humans suffer, and the field is proud of this.
MR also highlights some related liquid fire from its comments section, specifically on first doses first.
Via same account, same energy:
Meanwhile in North Dakota, a ban on mask mandates. Gotta love the detail that the legislature uses a mask mandate themselves.
More data on who thinks we should wait until teachers are vaccinated, I continue to find it interesting that we rarely ask if they should fully reopen or not once all teachers who want the vaccine have received it, which is the question I’d be most curious about:
The Eyes Have It: Study suggests wearing glasses could reduce Covid risk by more than half. Proposed mechanism is that this avoids rubbing and touching the eyes, because everyone has to constantly use their purity instincts and blame touching things instead of the obvious explanation that glasses shield the eyes from airborne particles the same way masks shield your nose and mouth. Either way, this suggests eyes might be a more important infection vector than we’d realized, and provides even more emphasis for what you do mattering more than people realize. The other alternate explanation is that wearing glasses correlates with a bunch of other things, and those things reflect lower risk, which also seems highly plausible. I wouldn’t read too much into this but yes I would try to wear non-prescription glasses or sunglasses if I had that option. Lucky for me my eyes are terrible and this is well-covered.
Adding daily tests to border quarantines into zero-Covid areas like New Zealand seems like it more than passes every possible cost-benefit test, but even there, nope, not testing. They’re only now even testing those working the border on a daily basis. Meanwhile, Austria is now testing all schoolchildren twice a week.
Looks like drinking is actually down over the past year, although not for those 50+?
The right thing: Still available! Congratulations, Connecticut.
Even if things start to get worse again before they resume getting better, I’m hopeful that we’re getting close in general, and that we’re close to getting everyone who wants one a vaccine. In the meantime, Xkcd is at long last on top of my cutting edge pandemic-beating strategy.
I feel like crying in relief. The doubling time of the UK strain being 20 days instead of 10, the massive boost of vaccines from Pfizer and Moderna, and the FDA announcing that they will have a streamlined process for approving vaccine modifications for the new variants. Together those three pieces of news alone probably mean at least a hundred thousand lives saved.
It seems weird to me that so few people have emotional reactions to this type of news. We get worked up about one person getting stabbed or raped, but if a hundred thousand fewer people die from an infectious disease, most people don’t even celebrate.
The UK is rolling out twice weekly lateral flow tests quite widely:
Anyone who wants it (mainly for those who work outside the home)
All Secondary school children
All school staff
Parents of primary and secondary school children
That seems like a really good thing. My worry is that a lot of parents will skip it because nose swabs are uncomfortable.
Though becoming less uncomfortable. Regulation/manufacture is belatedly catching up to the idea that you can take a swab from the front of the nose, which is MUCH more bearable.
Updated post to include a prediction for next week, which I forgot to do. Prediction was made at 9:10am eastern on Friday (so it involves seeing Thursday’s numbers).
Just to check, do you want us to reimport, or did you do it yourself?
Did it myself, if I want a reimport I will say so explicitly.
I first read this sentence as suggesting that killing people is the best way to prevent infection.
Yes, apparently death is the right answer, either way. ;-)
On wearing glasses: Do you think contacts would also be helpful?
I’ve noticed, for example, that my eyes aren’t nearly as affected by chopping onions when I’m wearing contacts. That seems vaguely similar to COVID transmission by aerosols.
Nonzero helpful almost certainly, also almost certainly much less effective than glasses.
Isn’t the exposure route drainage ducts that feed into the nose and lungs? The cornea isn’t living in itself, it has no cells for the virus to afflict. The contact is only covering the cornea, while glasses are acting as a “shadow shield” to reduce the number of droplets that hit the eyes.
In light of this likely mechanism I would not assign “almost certainty nonzero helpful”
The slow decline in deaths seems like it must be primarily due to delayed reporting.
We know that there were a few big batches of delayed reports, plus day of the week effects. I can’t think of a good reason to expect those without also expecting a significant number of small batches.
I expect that hospitalization data is much more reliable evidence about the timing of bad health. It shows the expected sharp drop. It also dropped faster than the death rate after the summer wave, and maybe slightly faster than the death rate after the first wave.
In order believe that the death rate was dropping much more slowly than the reported hospitalization rate, it would seem to require something like deaths per hospitalization rise as hospitals become less overwhelmed, or that there are reporting problems that have a significant effect on the rate of change of hospitalization data. Neither seems likely.
I suppose there might be some predictable demographic changes that alter the death rate (i.e. younger people get infected at earlier stages of each wave), but for recent data it’s hard to reconcile that with the effects of vaccines.
It’s got to be either reporting delays, or people dying months after they contracted the virus. I’ve changed my mind a bit, and I’m currently guessing it’s more the latter.
I compared the ratio of reported deaths over the past week in California (1273) and New York state (406). This clearly has no connection with people who recently tested positive, since New York has been reporting over twice as many new cases as California recently.
It was only before mid-January that California last reported something in excess of twice the new cases that NY reported, and only around Christmas or earlier that California reported 3 times as many new cases a NY.
So unless there’s something quite misleading about the ratio of California to NY numbers, recent deaths are dominated by people who contracted the virus around Christmas / New Years.
I can test that hypothesis a bit more robustly but I think this requires the delays be longer than they previously were.
What do you think of the John Hopkins tracker?
Recently many sources have reported a “CA variant” with many of the same properties as the English and South African strains. I haven’t personally investigated, but that might be something to look into. Especially given the number of rationalists in CA.