A massive waive of cases continues to hit China, as one would expect given last week.
There is also a new variant, XBB.1.5, that is spreading rapidly starting in New York, so it’s time once again for our favorite game show, ‘how much trouble will this new variant cause?’
The Twitter Files finally got to the part about Covid censorship. I will discuss this later in its own post, hopefully tomorrow, if not then next week. It did not seem worse than I would have expected.
Executive Summary
XBB.1.5 is coming with a large reproduction advantage, peak will likely be later and larger than it would have been otherwise.
Everyone in China is getting Covid.
The Covid edition of The Twitter Files will be covered on its own.
Let’s run the numbers.
The Numbers
Predictions
Predictions from Last Week: 410k cases (-4%) and 2,500 deaths (-7%).
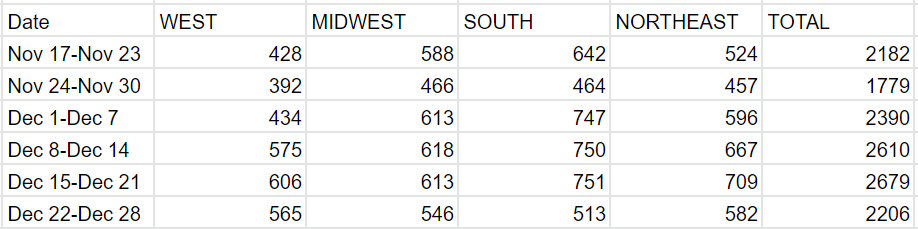
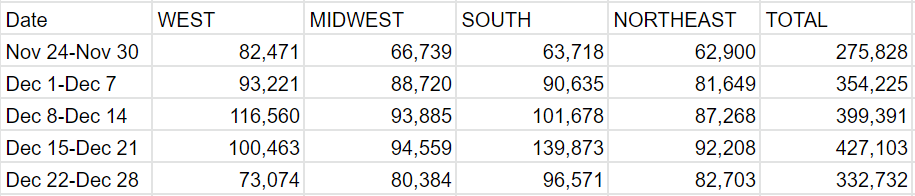
Results: 333k cases (-22%) and 2,206 deaths (-17%).
Predictions for Next Week: 385k cases (+16%) and 2,600 deaths (+17%).
I intentionally didn’t fix any reporting issues this week other than Florida. It seems I underestimated Christmas being a special thing. That’s on me. It doesn’t have an impact on the underlying situation. My presumption is reporting will catch up over the next few weeks, but New Year’s is still a thing so not fully back to normal yet, and a lot depends on decisions in various states and my decision on which ones to patch versus not patch. The real prediction is small overall real growth in cases, with the Northeast seeing the larger real increases.
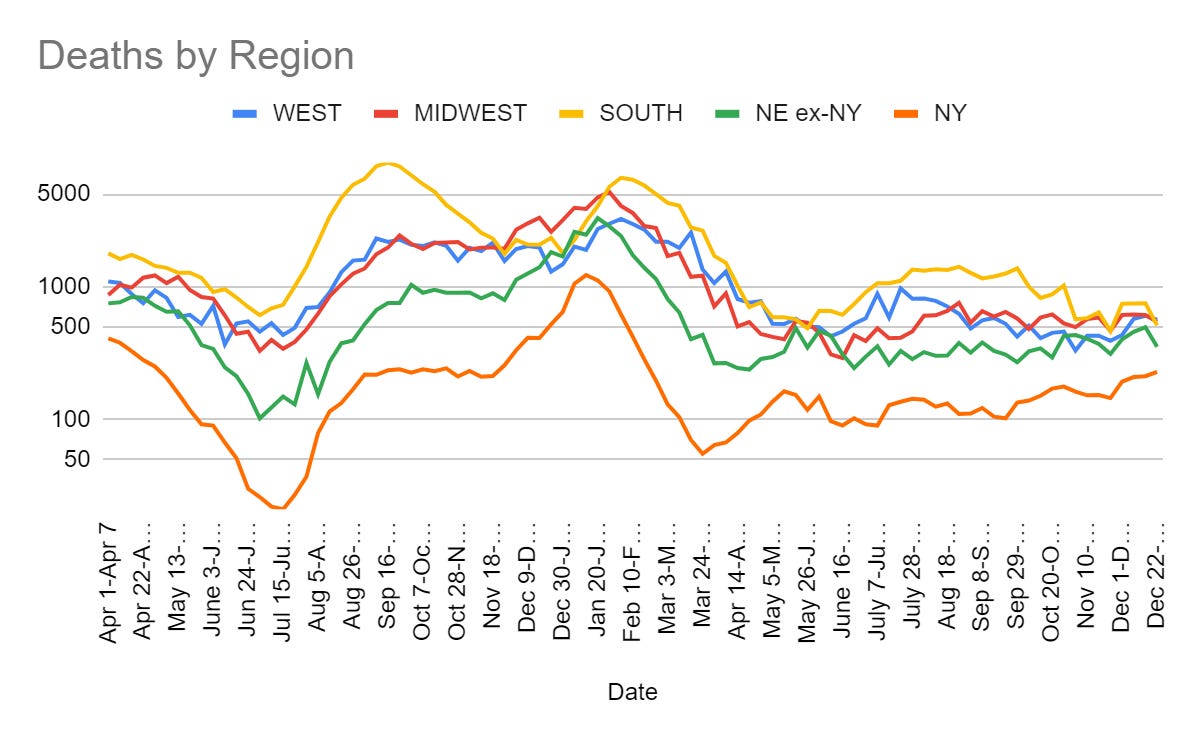
Deaths
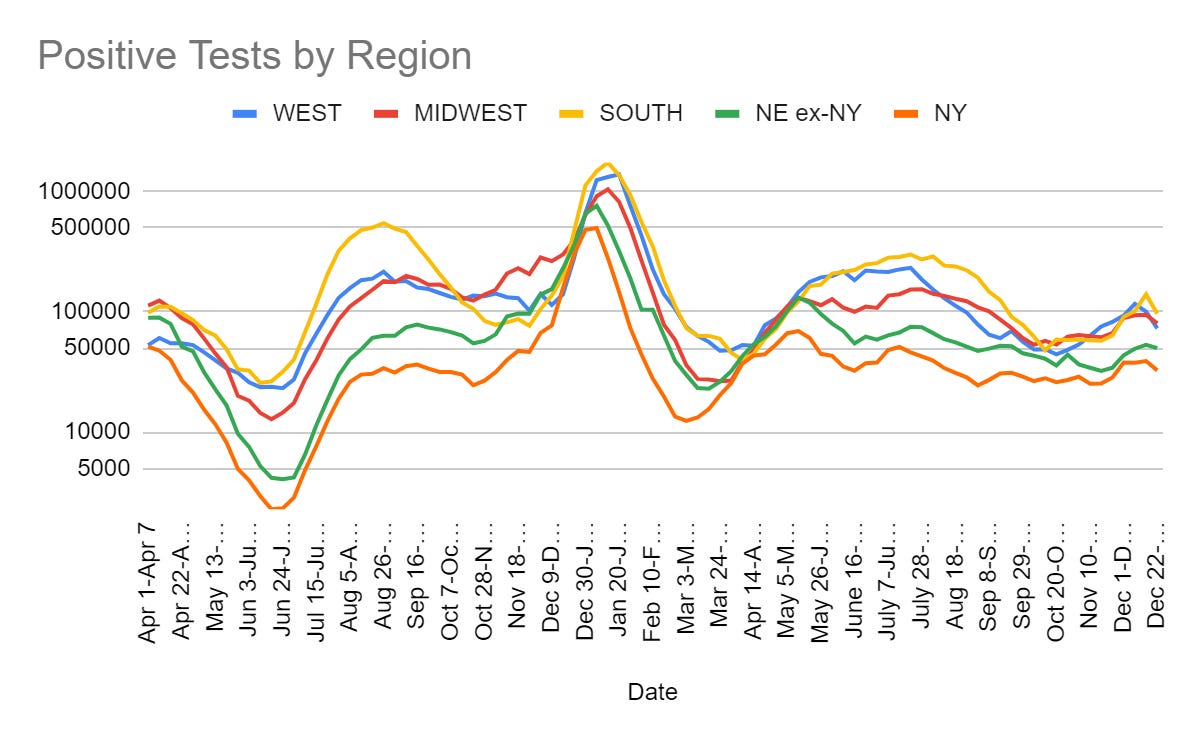
Cases
An interesting twist is that California was down by a third and they report on Fridays, so that shouldn’t have been impacted by Christmas. North Carolina and South Carolina took the whole week off (as did Florida but they only report every two weeks anyway so I patch them every week).
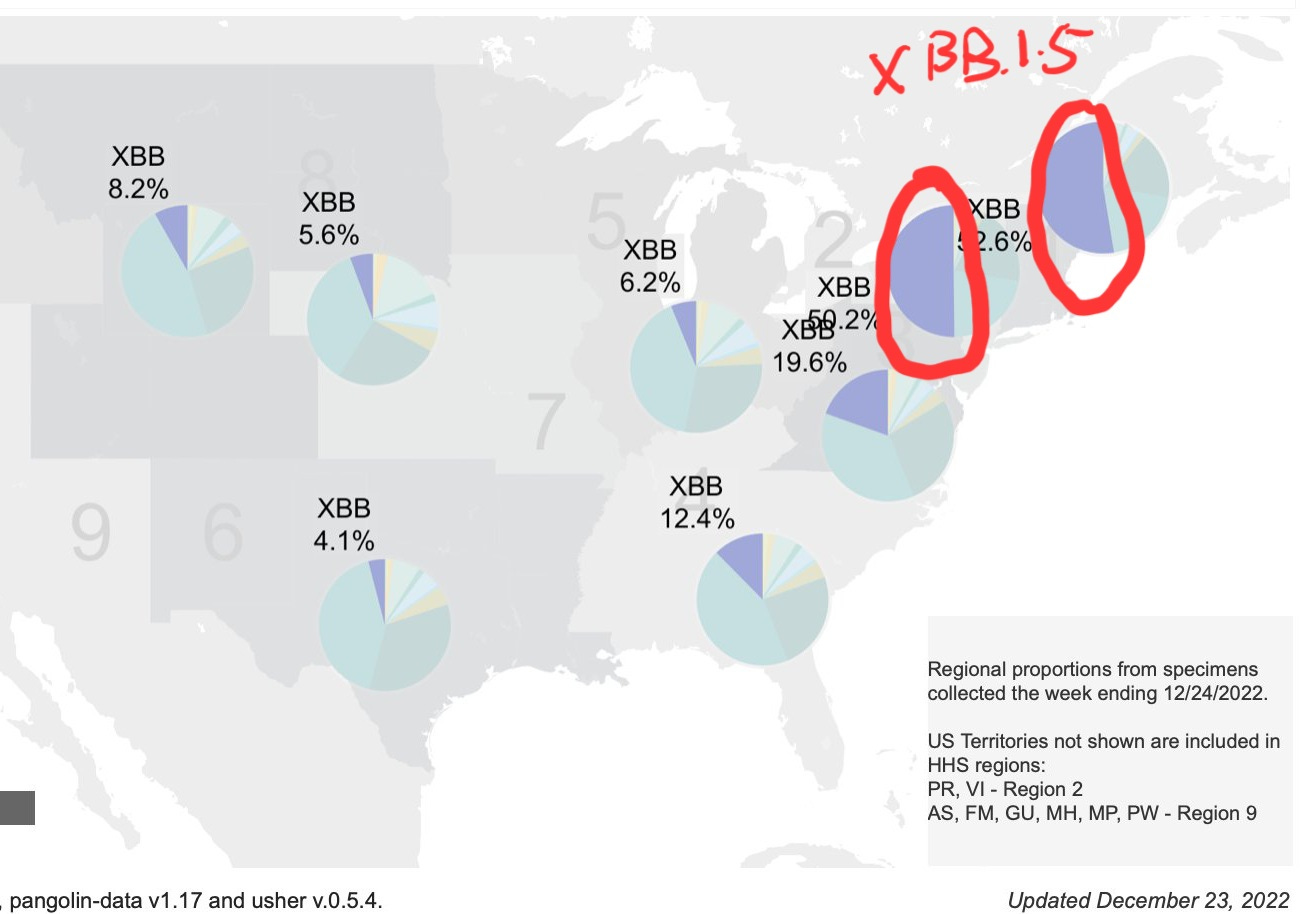
XBB.1.5
Here we go again, as usual I am editing the thread down somewhat.
Note that Weiland here uses weekly advantage of the new strain. That’s going to be higher than a variant’s advantage in terms of percent of new infections from a given case, so ‘108%’ or ‘120%’ or ‘700%’ is still big, but not as big as it sounds.
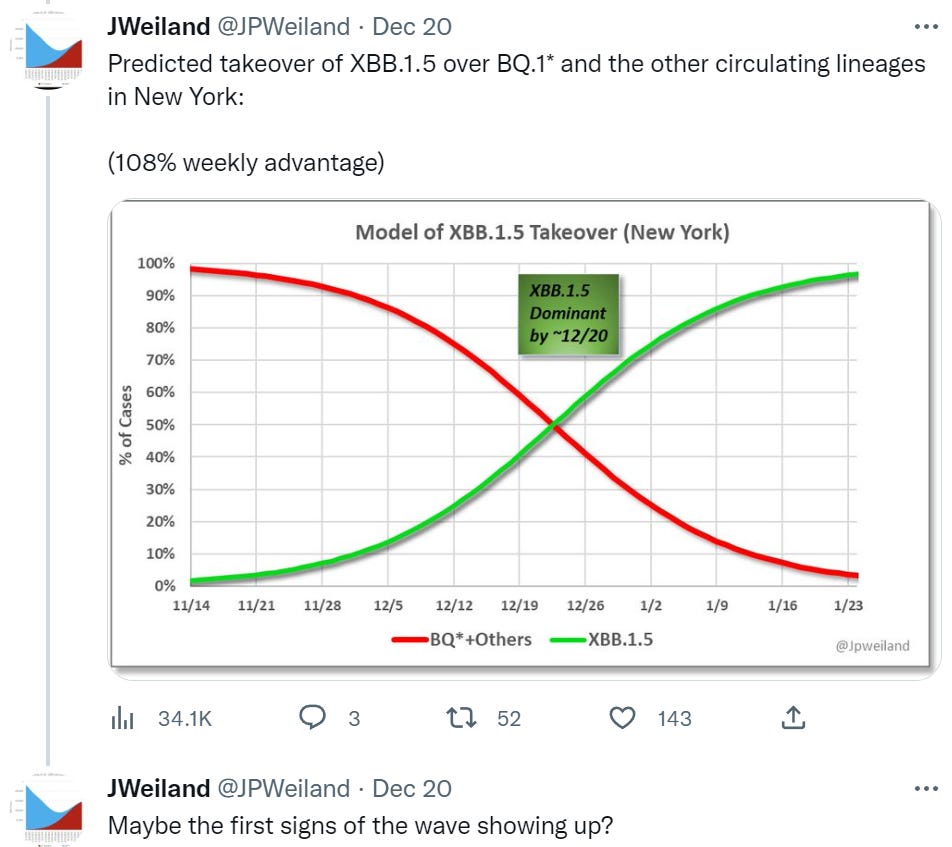


This chart from Bedford uses the terminology and scale I’m used to using.
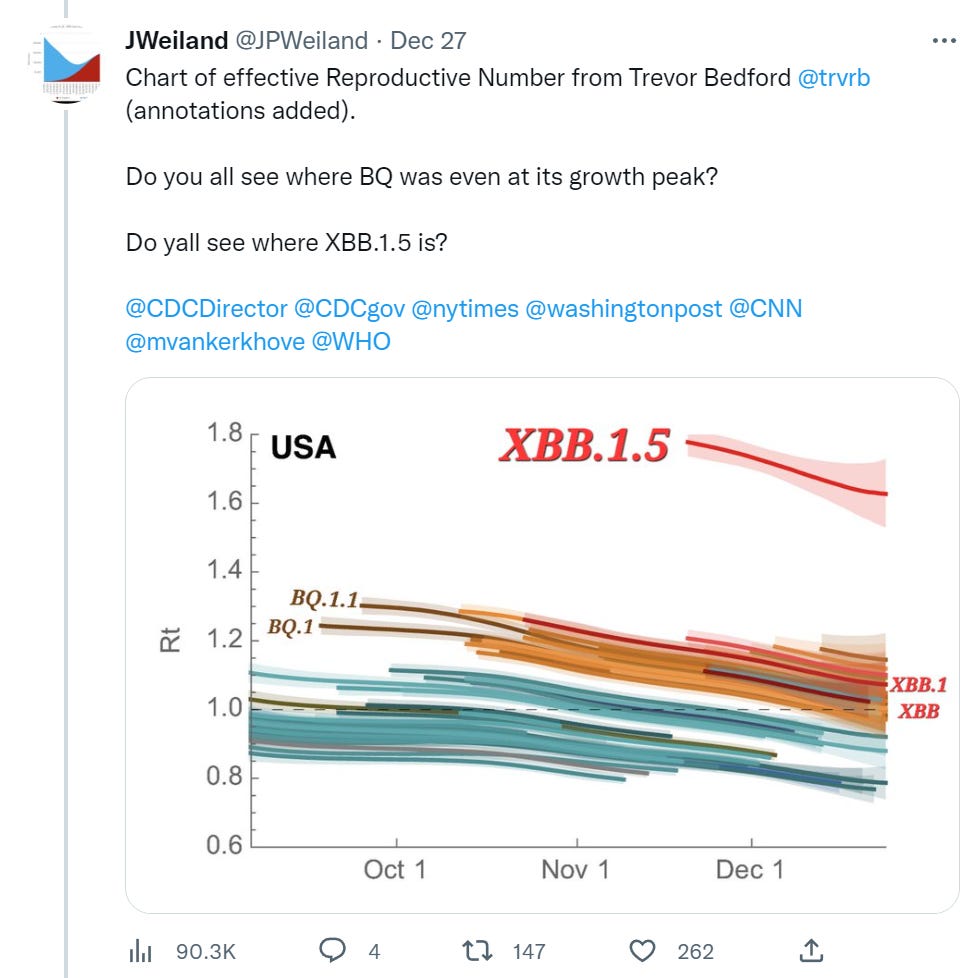
How many Omicron variants in this subclass is this now? At least four.
The framing of ‘the middle of a BQ wave’ is a lot of what holds me back from overly worrying in these spots. Is this a BQ wave? Technically, sure. In practice, this felt much more like a December wave, and BQ happened to be the top variant at the time.
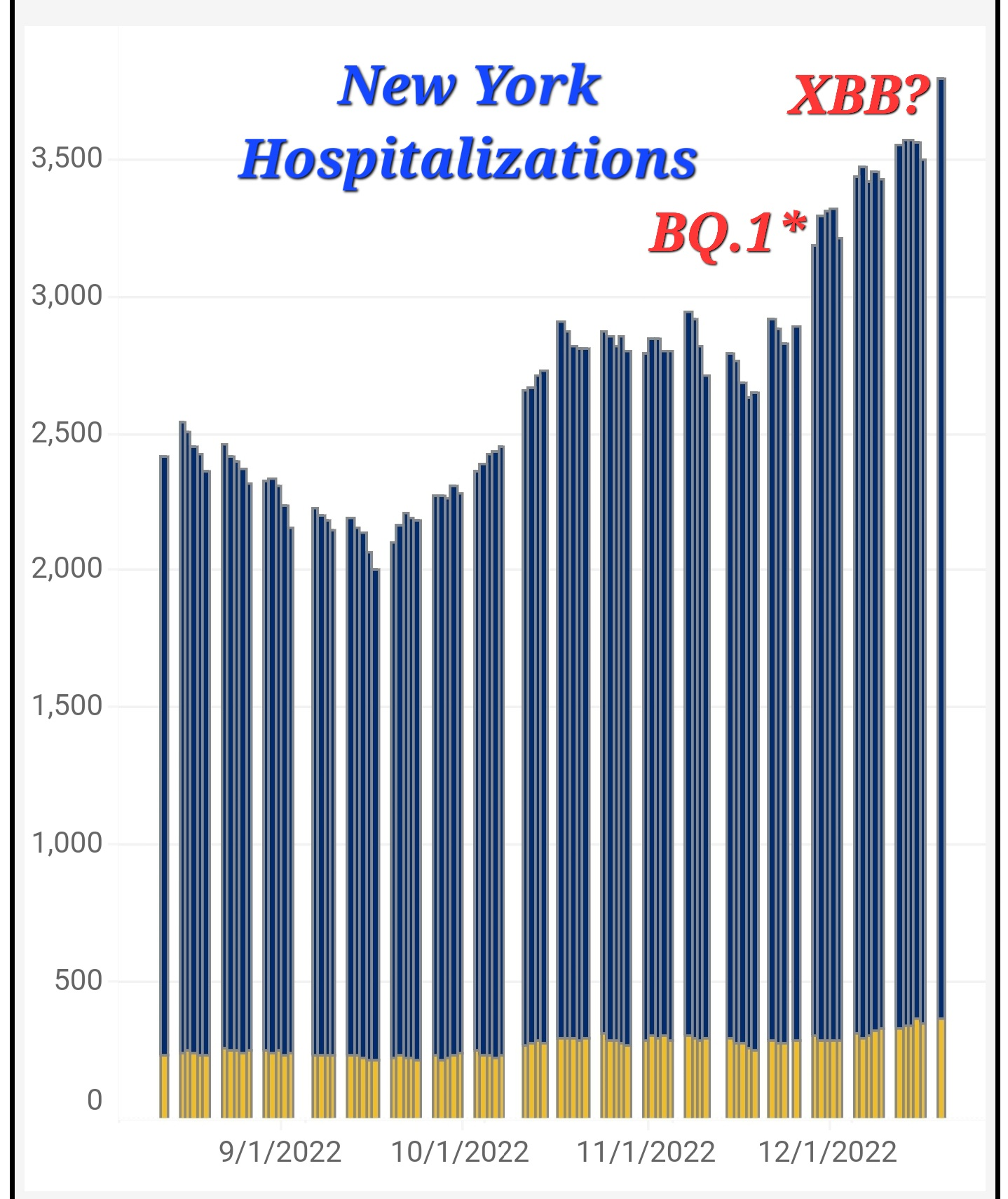
XBB.1.5 is coming in strong here, with a modestly larger initial comparative advantage over its predecessor. There’s still a long history of such advantages fading with time as the population adapts and conditions change. Instead of happening at a time when a wave is natural, this will come at a time when a wave would be going against the natural flow.
Note that in at least New York a majority of cases are now XBB.1.5, which means this is already a ‘XBB wave’ there, and that it materialized, one more time, out of very low numbers, once again showing that our decisions have little long-term impact on the flow of cases except insofar as we cause or prevent new variants.
My guess is this effectively prolongs the high-cases period for a few additional weeks, with somewhat of a second peak, and means New York and the Northeast will get the second peak faster and return to baseline levels faster.
What would a ‘functional CDC’ do with this information? Should we shout it from the rooftops? What would a resident of New York do with this information? Should anything change at all?
It seems to me like the clear answer is that very little changes. Some medium term planning of when to schedule highest-risk activities or expect more people to become sick changes.
I do not see anything along the lines of ‘we need to prepare hospitals’ or ‘people should largely be modifying their behaviors.’ Yes, there is a new variant, and things will be worse on the Covid front for a bit than they would have otherwise been. No, this is not a cause for alarm.
I agree that the contrast between BQ (lots of hype) and XBB (no hype) means a mistake was made somewhere. I think the mistake was with BQ.
Physical World Modeling
Excellent news: Generic massively cheaper Paxlovid is on its way.
Bob Wachter thread lays out his full current algorithm for Covid risk mitigation, and there’s a follow-up thread as well. It takes advantage of the ~50% heuristic, that a lot of interventions, like recent booster, good ventilation, masking or rapid testing, each lower risk ~50%. The exception is KN95s which he has at 90%+, and he sees a well-fit N95 as neear-100%, so he’s basically fine with anything while wearing one. If he wants to avoid using a KN95, he then asks whether he can get risk below his threshold, given background conditions. Very high effective estimates here.
Given his physical model, this all seems like a reasonable compromise, provided the threshold is well chosen. As you’d expect, I think Bob’s is far too high. Also it needs to adjust for the value of the activity, as he notes with his mom. Bob notes that he’s equally often accused of being too careful and too cavalier, which is an interesting fact about who gets shown such threads and chooses to make such accusations.
What Bob doesn’t take into account is the background or general cost of being in constant calculation and mitigation mode, instead of being in live-your-life mode. I remember what that other mode was like. It’s a big deal.
Another study saying boosters work (study, second additional thread), this time enhanced neutralization against Omicron subvariants BA.2.75.2, BQ.1.1 and XBB. At this point the question to me is for how long they have these effects. Updated boosters would be well worth it if their results were permanent or largely lasted for years, mostly not worth it if they only buy two months given the next day side effects. So where in that spectrum are we? I’m not seeing good data.
Your periodic Long Covid reminder.

Except no, those are not the worst activists in the world. For example, they’ve got nothing on PETA. Activists use this level of obvious nonsense rhetoric all the time in service of lots of real issues and worthy causes, including those with the most pervasive activists. Where a normal person then looks around and says ‘my lying eyes tell me your loud super confident claim is obvious nonsense’ and then they tune the whole thing out. Would activists be better at improving or changing the world if they stopped doing that? Yes. Alas, pressures within activist circles will not allow this to stop.
Another reminder with a side of odd overreach.


I am frustrated by such people, yet I think that Christel is interpreting their statement incorrectly, and therefore misdiagnosing the whole ‘any kind of Public Health’ solution. We do indeed have ‘any kind of Public Health’ and in some ways they are making the problem worse.
The person saying their cold ‘turned into’ Covid does not mean ‘I caught a cold that was a different virus, which magically transformed.’
What they mean is one of two related things, both of which are valid.
The first meaning is ‘when you think you have a cold, be aware that it could be Covid.’
The second meaning is ‘beware getting tested for Covid, because if you test positive for Covid then you Have Covid and people will demand a different magisteria and order of magnitude of precautions and freaking out, out of proportion to the situation, that you very reasonably would prefer to avoid.’
A lot of people, at this point, consider the main downside of Covid the way people react to it, because in most individual cases, from an individual’s point of view, this is correct. This is wrong, because the tail risks are really bad. But I understand, and notice that public health can make this phenomenon worse.
Technical thread about why people shouldn’t worry about IgG4-related-disease and its relation to mRNA vaccines, in response to this study implying reason to perhaps worry. I am not an expert here and haven’t asked one, the thread’s arguments seem fine to me as far as that goes.
Permanent Midnight
I also predict few will be convinced here (link to article).

Be aware that these efforts continue, and that by the logic underlying Public Health left unchecked, ordinary life and its joys would cease to be.
In some places, this seems to be succeeding, such as in some dance events.
China
On December 23 from Scott Gottlieb: Situation on ground is far worse than official reports. He then notes, as such folks often do, ‘only about 70% of those over age 65 have been boosted, only 40% over age 80 fully vaccinated (note the interchange).’ It is amazing the degree to which, even with a different vaccine, lack of sufficient adherence to vaccination schedules is implied to be the reason there is trouble.
On December 23: China estimates 250 million people have caught Covid in 20 days.
China’s hospitals are at full capacity, patients can’t find beds. Whereas the commercial areas are full of people, either already recovered or young enough to take their chances. This makes sense – if estimates are correct we are talking about 3% or more of some regions being infected per day and that adds up fast, no reason not to then go back to normal. Whereas there is no hospital system on the planet with any chance of not overflowing under such conditions, even in the best case. This was not the best case. Hospitals had no warning and made no preparations.
Scott Gottlieb makes a scary point that China has a bunch of different variants spreading at once that don’t all provide that much cross-protection from each other. That means that means that not only will most Chinese people get Covid, it is plausible a lot of them will get Covid multiple times, and the acute phase of the wave could last for several months rather than cresting quickly.
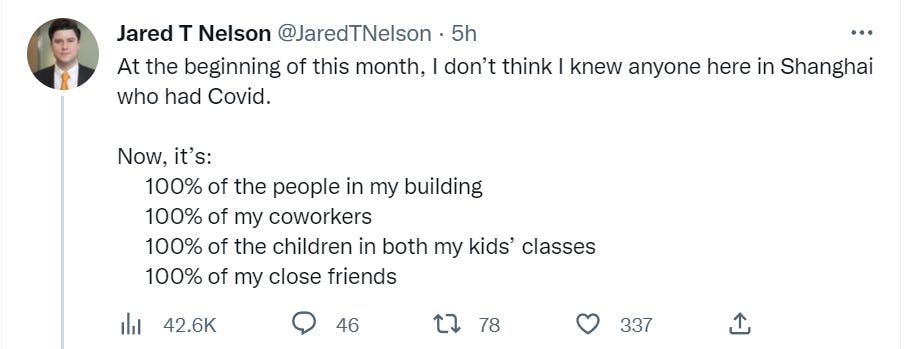
Jared Nelson, based in Shanghai and one of the handful of accounts based in China I keep tabs on, has his family all get Covid right at Christmas, as one more anecdote of how fast things are playing out.
He then updated from his family to everyone.

On January 8, China will end all quarantines, including for inbound flights. Flights so far have been scarce and expensive.
That means of course it is time for America to impose restrictions on travelers from China. Also Taiwan, Japan, India and Italy. It isn’t completely unreasonable given that it would be reasonable to estimate ~10% of Chinese people have Covid before they start traveling and a lot more by the time they exist their flights. The problem is America has fully uncontrolled spread and given those conditions Chinese travelers are not going to change the overall picture. We keep doing the same dumb things over again. The good news is this seems to only be a testing requirement, so it’s not so bad.
China previously called Covid a ‘class A’ disease like cholera or bubonic plague, justifying zero Covid. Now it is a ‘class B’ disease, which is not like that.
Basic over the counter medicines are essentially impossible to get. Paxlovid is in short supply and very difficult to get.
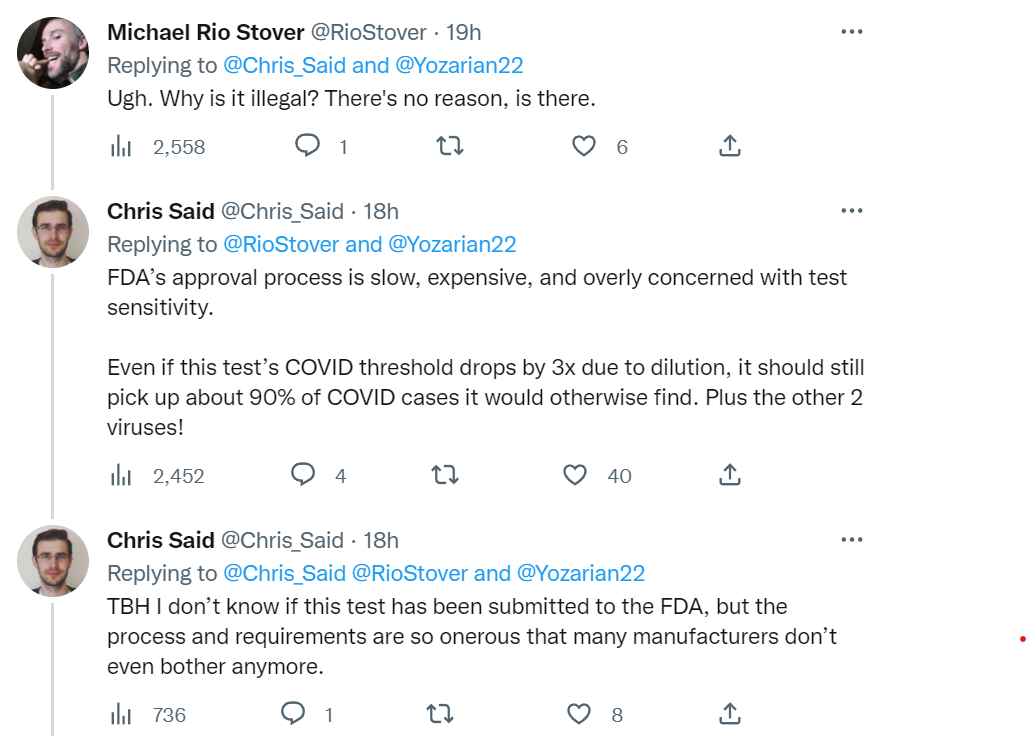
FDA Delenda Est
Forgot to include this last week, Alex Tabarrok reports on WSJ article covering the FDA’s attempt to gain authority to halt most progress and innovation in laboratory developed tests. There can be no doubt that allowing this would cause not only catastrophic delays in availability that would devastate patient care (read: kill people) it would also mean that many or most potential future such tests never happen at all, and when they do happen are vastly more expensive. If you’re reading, you almost certainly know why and how this would happen.

To be fair, rather than fly to Germany you’d presumably get a much more expensive and slower set of PCR tests.
Other Medical and Research News
In DC there is a human challenge trial (direct link) for Zika vaccine for assigned females at birth ages 18-40 who are very very sure they are not going to be pregnant in the next few months. I hereby endorse such efforts and commit to viewing anyone who participates like the badass they clearly would be.
Colorado decriminalizes DMT, mescaline, ibogaine and psilocybin.
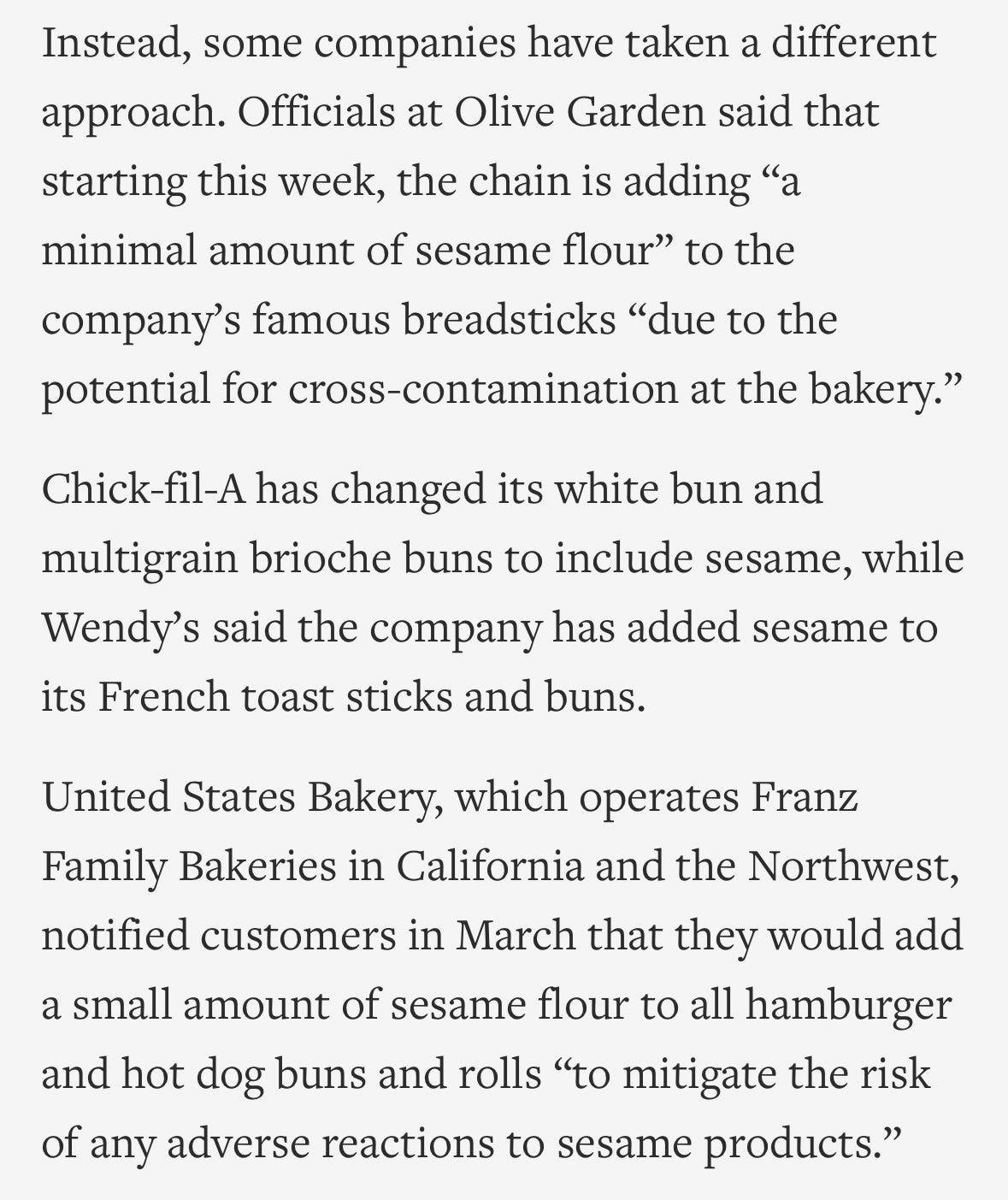
The law of unintended consequences strikes again. If you need to correctly label exactly which products have sesame in it because it’s an allergen, it is expensive to verify you can check the box for No and relatively cheap to ensure you are correctly marking the box for Yes.
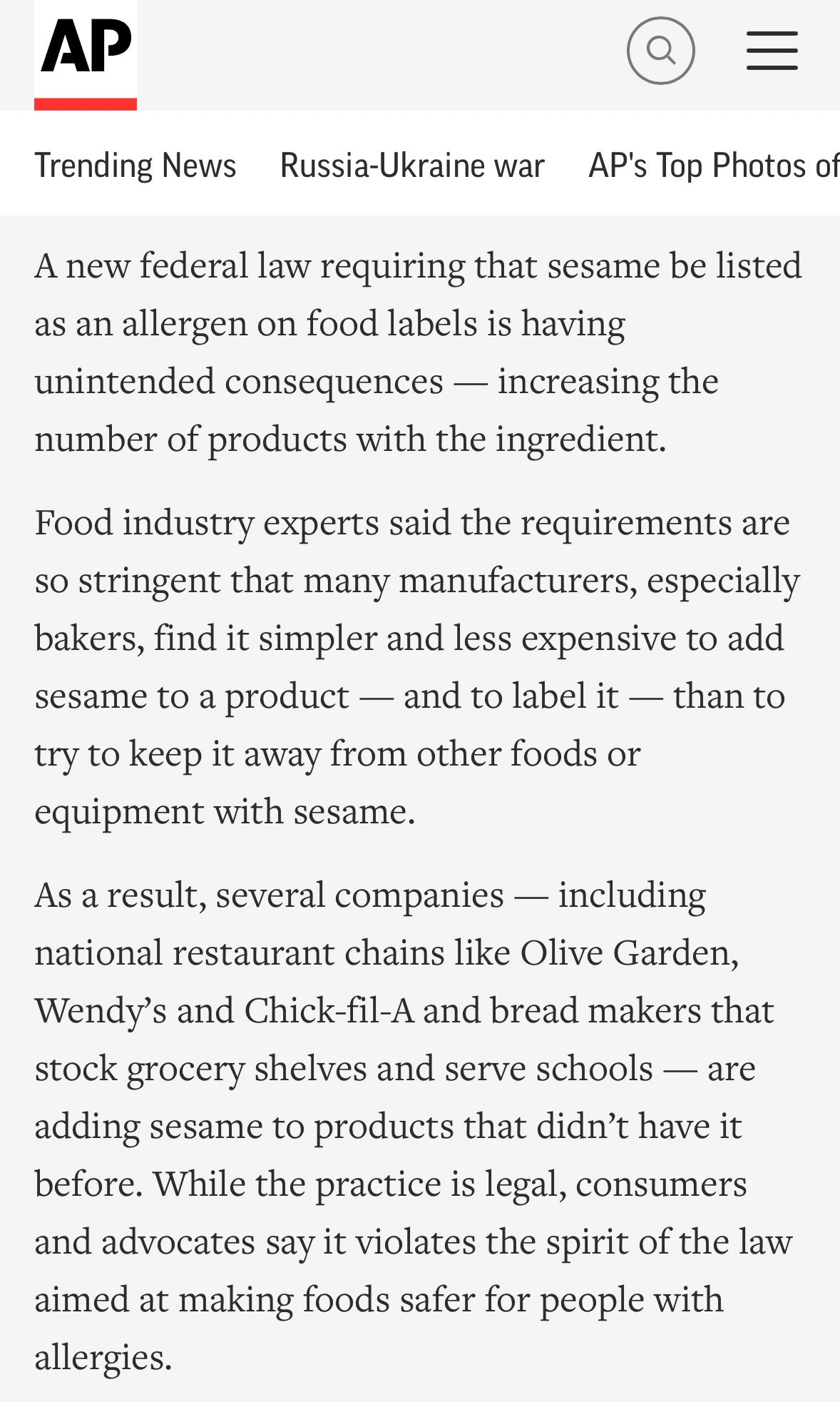
This generalizes.
‘Flu season starting to wane after brutal start, including at least 12,000 deaths.’ That is still on the very low end of the typical yearly death count (12k-52k). (In ‘GPT makes stuff up a lot’ news, ChatGPT said ‘over 40k according to the CDC.’)
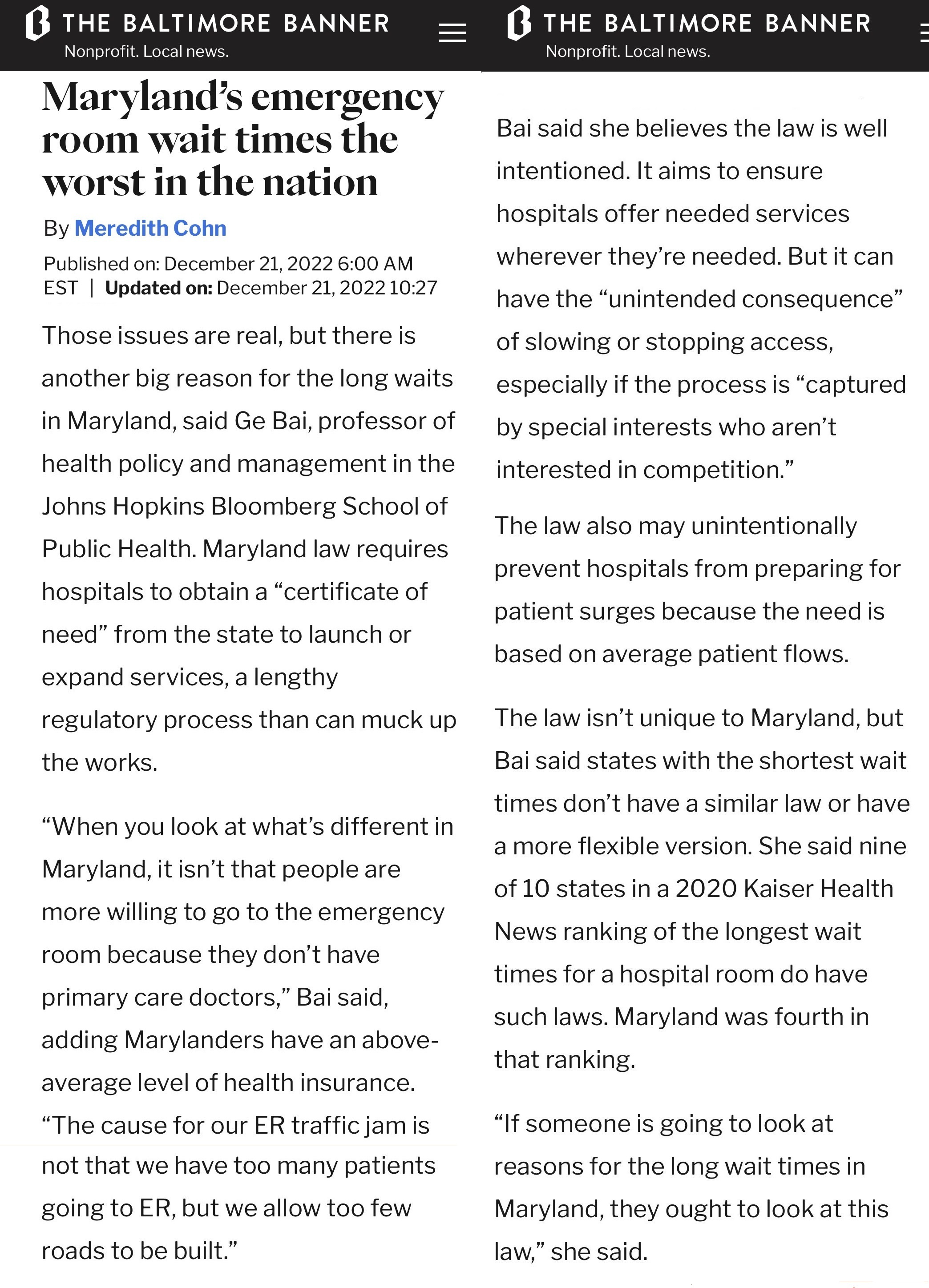
Maryland ER wait times average 228 minutes (direct), worst in the country. I presume this is for all reasons to visit combined, and those who need triage still get seen much faster. I also note that a few weeks ago we heard about the situation in Quebec and it was much, much worse there and also at least some other places in Canada.
At least some blame is being put on Certificate of Need laws, which require a hospital to get approval before they can launch or expand services. There seems to be a correlation between requiring Certificates of Need and… unmet needs.
Another possible cause are the price controls and fixed budgets. Article says one in four nursing positions remains unfilled, which typically indicates an inability or unwillingness to pay the going rate.


It seems highly plausible that combining ‘don’t allow expanded services,’ ‘don’t pay more money for more services’ ‘strict price controls on what you can charge for services’ would result in a shortage of those services, which then get allocated by willingness to wait. A lot in common here with the Canadian system, perhaps.
The law also may unintentionally prevent hospitals from preparing for patient surges because the need is based on average patient flows.
Nothing about this seems unintentional?
Other speculations cite a lack of resources to treat those with mental health issues and a rise in the share of behavioral admissions, which locks up emergency beds, and a lack of access to primary care. Neither seems to differentiate between Maryland and elsewhere.
Everyone’s favorite game show, Good News or Bad News? (direct original source)
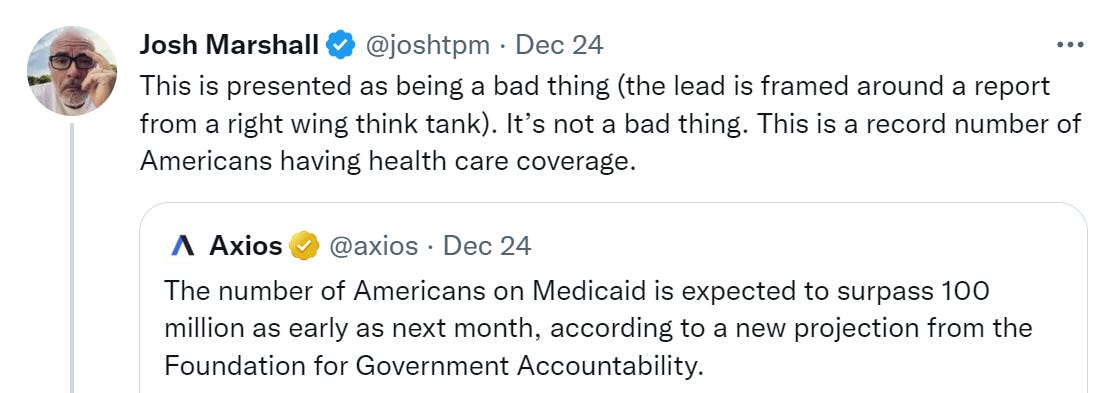
If you model this as telling you that people who previously would have had no health insurance now have Medicaid, while telling you nothing about those people otherwise, this seems like good news.
Not conditioning on this tells you that an awful lot of Americans need Medicaid and cannot do better. Which seems, if new information, like very bad news.
A Twitter thread dive into the history of various increases and cuts to Medicare payments, especially in regards to primary care, featuring several sequesters in various unintended states of implementation. It seems that Congress ‘finding a pay-for’ to justify their spending is a central motivation behind policy setting, so we systematically line up a percent cut in Medicare and other mandatory spending. Which we then sometimes waive later without paying for it, and sometimes meant to waive with or without a way to pay for it and end up doing anyway kind of by mistake and also kind of not.
Two reminders, one about therapy in particular and one about supply of high quality work in general.
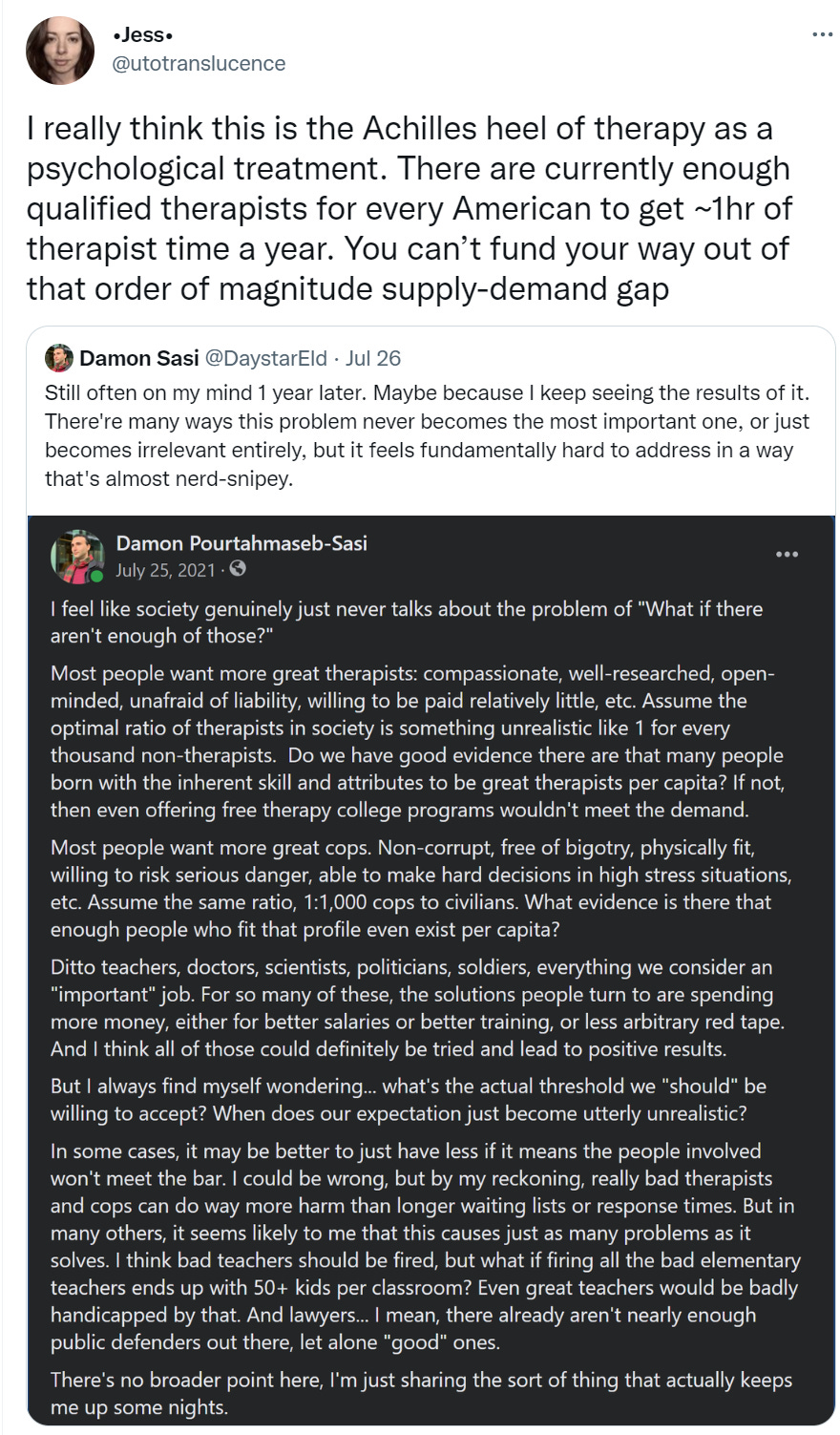
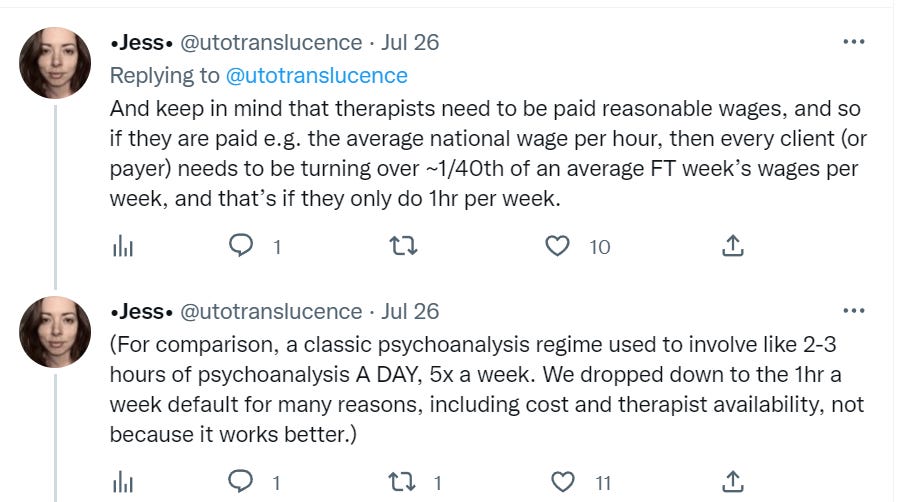
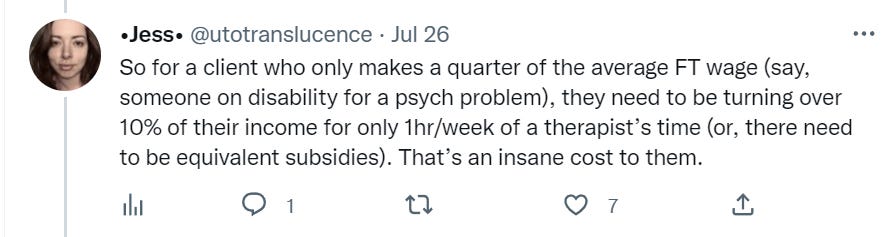
Even the current supply of quality therapists requires above average wages, and taxes are a thing, and few if any therapists can do forty good full sessions a week – twenty is more typical – so this is a several-factor underestimate of the costs if insurance or the government isn’t footing the bill.
In terms of physical time costs, this is not an 0.1% situation. We are talking about over 1% of the population as full time therapists. Is that something we could do? I think actually yes, if most of the patients were average people, that this is something that many people could do well and enjoy and get meaning from. I also think that we have enough bullshit jobs out there that we could make the necessary cuts to free up their time.
We would still have to both pay them enough to make that many people choose the profession, and offer them the necessary training and way to get started. Which would be tough.
Same goes for growing all the other professions listed, and many unlisted. However many jobs out there you think are bullshit, however bad you think our current implementations might be, there are a bunch where it is clear that at least when done well a lot of value is produced, and more people would produce more value.
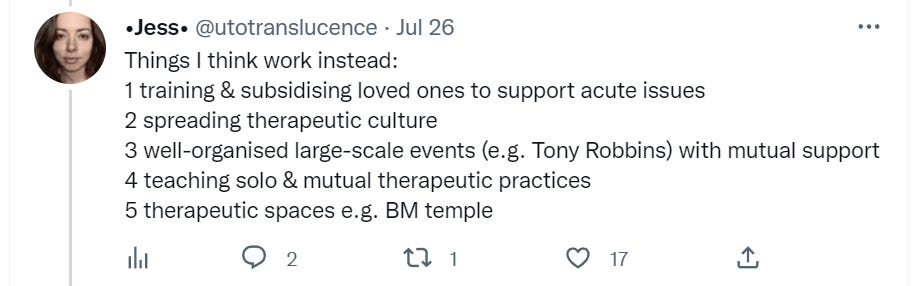
What are the most dangerous jobs?
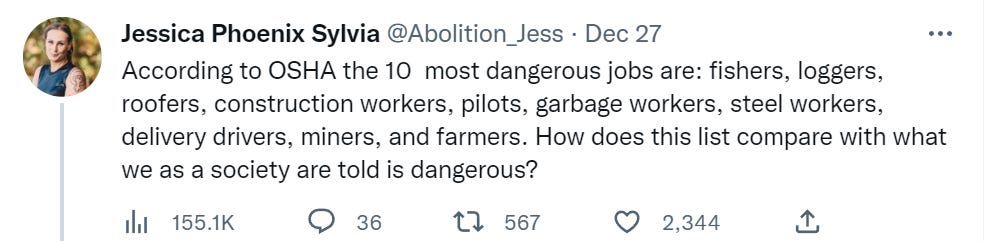
There is a clear pattern here. Accidents are in general far more dangerous than people. Police officer is at #25 surrounded by ‘person who is in proximity of potential accidents, especially with heavy equipment.’
Even if we knew, we likely would want to avoid changing our view of the risks involved, because we view accident and mechanical risk as unfortunate parts of life but different in kind to danger from other people. Especially bad people.
Yeah, the “what if there are not enough” problem. I keep saying this for years about teachers.
We want everyone to be educated. (I agree.) Ideally, we would like almost everyone to have an university education. And we want to have small classrooms, and individual attention to students. Also, teachers should understand their subject perfectly, and should be great with kids (ideally work with all kinds of disabilities).
And I am like: yeah, but that would require X% of population (depending on your ideal classroom size) to become teachers. Do X% people even have the desire traits? What if they don’t? (Also, not everyone who could be a teacher, should be a teacher—we also need people who are great at something to actually do it, as a job.)
But instead of thinking about the constraints of the problem, the answer is that we absolutely must to have everything. And the reality is that some schools have great teachers, many schools do not, and the parents who are aware of this compete for getting their kids into the right schools, while everyone loudly insists that no such thing is happening, because all schools are great… or at least, they should be.
There is a third option, one that fits in nicely with your view of bureaucracy.
The rules for Medicaid enrollment changed: The Families First Coronavirus Response Act COVID-19 Public Health Emergency Unwinding FAQs (medicaid.gov) requires that Medicaid programs keep people continuously enrolled through the end of the month in which the COVID-19 public health emergency (PHE) ends. The numbers are at a record high because new people are added, but the old ones don’t leave. And there is no plan to end a public health emergency that justifies expanded government.
Antivax sites are talking about similar results as indicating that the vaccines are inducing tolerance. Do you have anything that would debunk that claim?
Ok, found a twitter thread which includes the claims:
and
If both of these are correct (IgG4 doesn’t prevent clearing of the virus or increase severity relative to other antibody profiles), then it seems to me that there should be no problem. However, I don’t see a citation for the “not seen clinically” claim, which raises a question as to how I’m to interpret it:
If it means that Sabina Vohra-Miller has seen an actual study that compared people with high IgG4 vs others and found that high IgG4 was not associated with any less effective clearance of the virus, and either forgot to cite it or I missed it among the other references, that would be reassuring.
If it means that Sabina Vohra-Miller looked diligently for any study that would find a result either way, and didn’t find any, or didn’t look and just assumed that she would be aware of any effect if found, that would be much less reassuring.
Since Sabina Vohra-Miller’s citations were inconveniently in image form, included below to save anyone else from OCR’ing or typing them out:
(I found the link to the above twitter thread from a comment at this antivax substack)