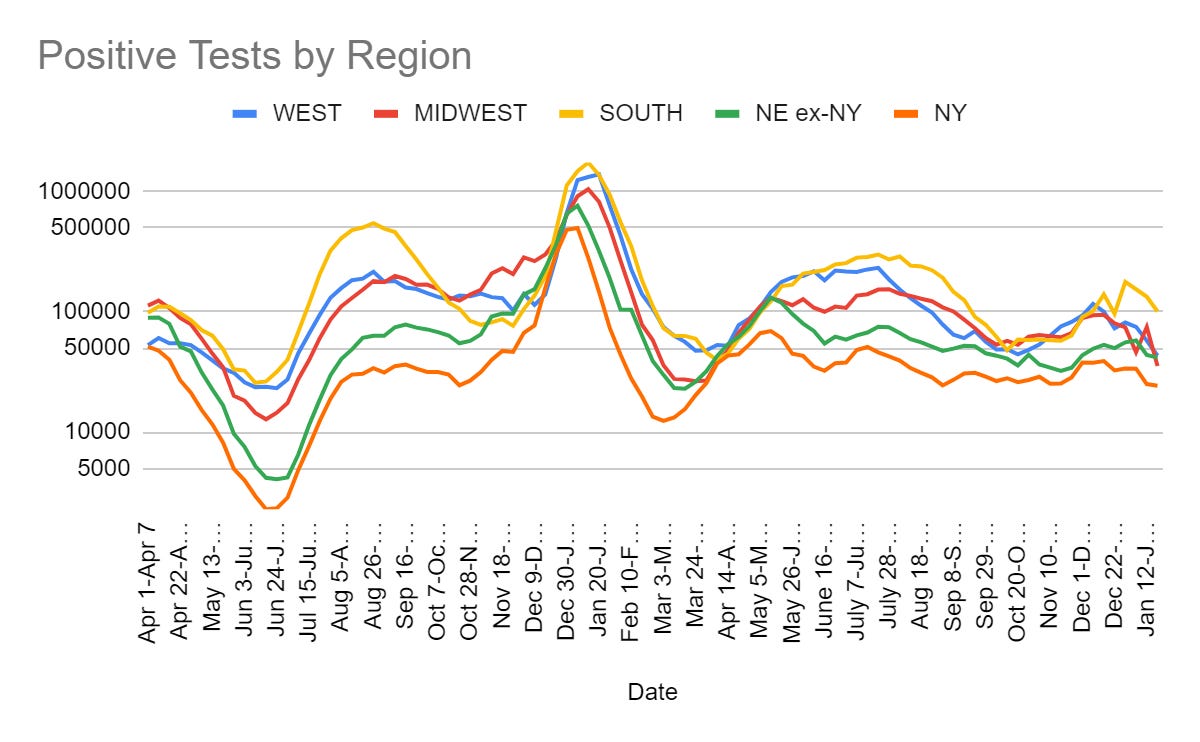
A large decline in cases, right at the end of January.
This week’s fun exercise is the clash between a call for the CDC to focus on being a center for disease control and offload its quixotic side quests, versus a former head of the CDC insisting that people will die (die I tell you!) if such dangerous changes are implemented.
Executive Summary
Cases down by 27%.
Former FDA head calls for CDC to be CDC, former CDC head returns fire.
Jury duty? School? Covid positive? No problem, come on down.
Let’s run the numbers.
The Numbers
Predictions
Predictions from Last Week: 320k cases (-5%) and 3,600 deaths (-8%).
Results: 245k cases (-27%) and 3,456 deaths (-13%)
Predictions for Next Week: 223k cases (-10%) and 3,300 deaths (-4%).
That is a huge case decline. Illinois did not report, although Indiana did – if Illinois does this a third time I’ll start correcting it the way I do Florida, for now I am not doing so. Most of the decline seems genuine, or a reflection of the end of some sort of backlog being filled perhaps. I am going to mostly buy it, and say that once again the seasonal peak has been reached. Things should improve from here.
Deaths also declined, which gives weight to the reporting hypothesis. They should start declining in earnest soon.
Deaths


Cases

How many cases are we missing? A lot. Here’s a fascinating chart of which cases are less likely to be reported by age and gender.

Physical World Modeling
Paper with details about the evolution of Covid variants. Has lots of technical detail, but nothing that changes my overall big picture views.
Bob Wachter sees conditions improving, is (somewhat) loosening up his rules.



Simplified Booster
FDA is proposing an annual Covid booster shot matched to current strains. If ‘current’ can actually be current, then this seems like a plausible best we can do in practice. It would be better to do this in response to important new strains but I will admit, essentially, good luck with that on multiple levels. Once a year might be doable, and should maximize total engagement. All the talk over the evidence required for new boosters makes me think all boosters will forever be out of date, so it will be a question of who wants an annual booster anyway.
There is also mention of moving to a single-dose initial vaccine, which isn’t explained and which leaves me confused on what they are thinking there. Certainly I can see spacing the two doses out more but the evidence for the second dose seemed very strong.
Celine Gounder also has additional details.

Are we still this stupid? An extra booster for the youngest of children?

If the public health system is to regain our trust, it needs to address the systemic issue that is still causing systemic pushing of prevention measures onto children at virtually zero risk from Covid-19.
Speaking of us being this stupid:

I do not think we should let this lack of funding allocation much impact such decisions. We should plan the sensible thing, whatever that may be. If we don’t have money to pay for it, perhaps we should charge money to pay for it?


Yes, that does seem like a good idea. Let’s do that.
In Other Covid News
We really don’t care about Covid at this point. For example, it does not get you out of appearing for jury duty.

As I can confirm as a parent, The New York City Department of Education’s new Covid strategy for classroom infections is We Don’t Talk About Covid.

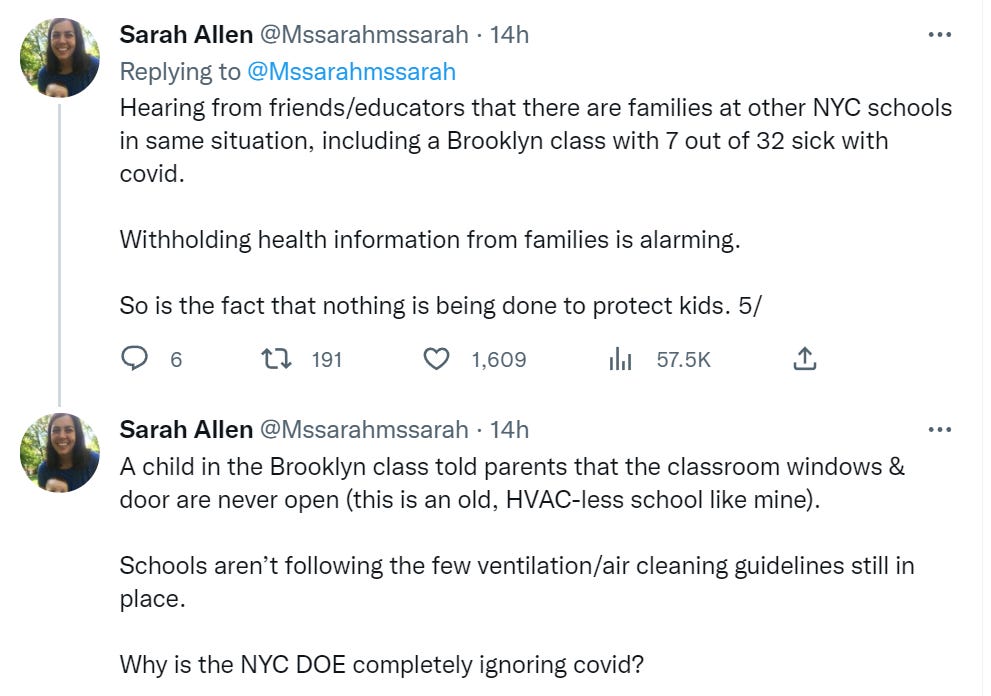
At the start of the year, we would get continuous alerts that some child, somewhere in the school, had tested positive. Now we get no information at all. Your classroom could be full of Covid cases, and they are not allowed to tell anyone.
Meanwhile, in other circumstances, we get the opposite situation.

It is Obvious Nonsense to turn away parents for not presenting vaccine cards, while also not alerting parents when a fifth of their child’s class is sick with Covid. The rules are not intended to make sense, they are a patchwork of improvisations and compromises.
Remember
In case anyone did not know this already or needs a reference for it: No, we are not hiding year-delayed huge vaccine side effects, this is all Obvious Nonsense. Those defibrillators they have everywhere have been there for a long time. Heart attacks have been common, including among athletes, for a long time. No, a bunch of people aren’t suddenly dropping dead, a bunch of people are cherry picking data. And a very clear explanation of exactly the level of Obvious Nonsense to assign to the completely false ‘athletes have 38 times as many heart attacks’ statistic.
Every so often, I get someone going ‘yeah you dismiss all the bad evidence for vaccine side effects (or Long Covid), but clearly you are cherry picking and ignoring the good evidence, what about this set of good evidence?’
I’ll then look at the information the way I would if something similar came up in my other information sources (note that if the link is to a video, this means almost certainly ignoring it entirely), and move on.
As usual, you have the option of hiring me at $500/hour to look into such claims and evidence, but I highly recommend you do not waste your money on that.


And I’ve never seen someone say “you know what, I was too reluctant to engage in this hot-button policy controversy.” Now obviously if you play it safe all the time, you reduce your odds of stepping in it. But I think erring too far in the other direction has its own costs.
I’d like to fix that. Anyone attempting good calibration is going to be too reluctant a good portion of the time. Whether or not I have good calibration, I am no exception.
So, with regards to the questions of the initial response to Covid, school openings, the need to repeal mask mandates, FDA Delenda Est, CDC Delenda Est, and honestly more things I end up mentioning than not, and obviously a bunch of things I end up not mentioning at all, and you can quote me on this:
You know what? I was too reluctant to engage in this hot-button policy controversy.
Ban Gain of Function Research
Some marginal good news on this front, for once: Republican senators introduce a bill that would create a moratorium on federal funding for gain-of-function research on potential pandemic pathogens.
We must be vigilant, they remind us, about taxpayer dollars. The important thing about creating the next pandemic is the same as the important thing about preventing the next pandemic, which is making sure our tax dollars do not pay for it.
Delenda Est Battle: Former CDC Head vs. Former FDA Head
Scott Gottlieb suggests fixing the CDC by focusing it and its culture on its core mission of disease control and transferring its other operations to other agencies, and outsourcing things like creating tests to private vendors. Seems like a great start.
Former CDC head Tom Frieden responds on reforming the CDC. He’s against it.

I notice up front that there being this many errors each of which is ‘particularly’ dangerous sounds a lot like protesting too much. Even if Scott Gottlieb was making mistakes, that is quite the accusation for suggesting shifting tasks to other agencies. We all know what this brand of talk is designed to do.
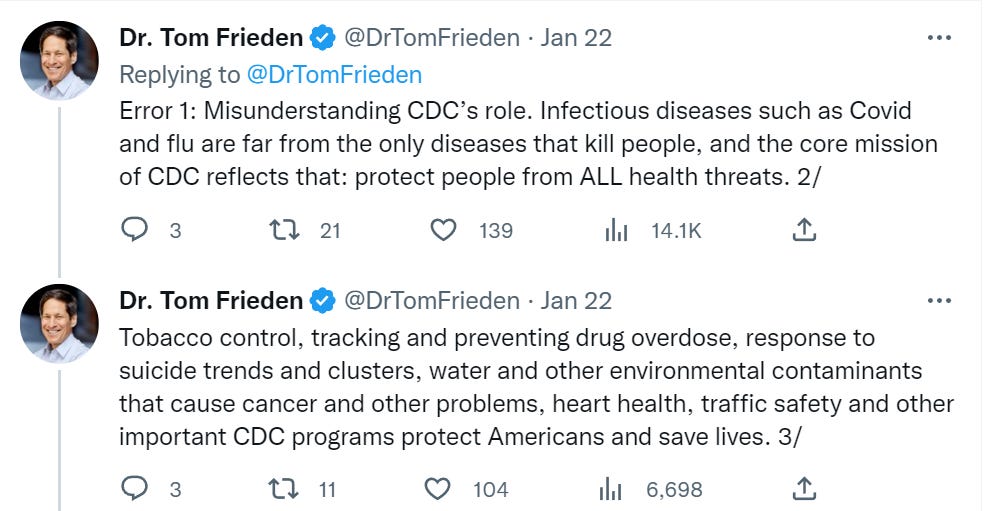
That’s… not… a Center for Disease Control. We have this thing called the Bureau of Alcohol, Tobacco and Firearms. The FDA regulates tobacco products and drugs. We have an environmental protection agency for contaminants. And traffic safety? Seriously, what the actual f***?
This is exactly what Scott is complaining about and says needs to change – an obsession with anything that can be called a ‘safety’ issue being brought under the banner of an agency no longer focused on its actual very important mission.

This seems to conflate the question of having experts on hand to understand these questions, and attempting to intervene directly in those questions. Unless I am very mistaken, no one is saying the CDC should not have access to experts in reproductive health. We are saying that perhaps another agency should be in charge of general reproductive health issues.
Whereas this by Frieden is a fully general argument that everything everywhere is the purview of the CDC, because socio-economic status impacts health outcomes, which impact disease outcomes. They ‘can’t ignore’ such factors, you see. Which is why they should be deciding whether or not people have to pay their rent. I really wish that was me making that example up. Somehow I am not doing that.

The CDC, once again, literally issued a regulation against evicting people from their houses. This is saying the CDC does All The Things. Scott is saying that the CDC should hand off many of those things. I don’t see the error here.
Oh come on. The FDA and CDC both do that, it’s duplicative and it’s stupid and the job should clearly belong to the FDA.

I am confused. The CDC made a mistake trying to manufacture a test? What was the mistake? Was the mistake forbidding everyone else from manufacturing tests, or was it only that there were almost no tests that also didn’t work?
And the CDC is continuing to work hard to develop similar new tests for future diseases? And challenging this is a ‘dangerous’ error?
I agree that such standardizations would be worthwhile and we should do them. I don’t see why this represents a dangerous confusion on anyone’s part.
What about the actual reform efforts of the current CDC head?
US public health chief Rochelle Walensky continued reconfiguring her agency to fight crises after stinging criticism of its pandemic response, hiring new leadership and creating new offices to address health equity and surveillance.
I notice this is all about creating new offices and hiring new people. There is no sign of anything that the CDC is planning to stop doing. This is not about focus and getting away from the wrong things. Instead, the manager must expand her realm.
As focus goes, how does this look?
Surveillance seems like a good place to focus. I continue to fail to pass the Intellectual Turing Test on the benefits of ‘health equity’ or why choosing it over making more people healthier doesn’t make you exactly what one would think it makes you. See the example of our vaccine distribution as documented by Patrick McKenzie, where we chose ‘equity’ over people not dying, and it translated in practice to ‘those who know how to work the system got priority.’
China
Head of Chinese CDC estimates 80% of country already infected. Whether or not this makes a second wave possible depends on whether there are multiple sufficiently distinct strains that don’t give enough cross-immunity, so it still might be possible.
Their CDC’s current estimate of cases is 280k a day, with 896 deaths. Numbers this low, this soon, do not seem plausible.
Travel without testing is over in China, worth remembering that there were many predictions this would never happen. Government did give up that opportunity to permanently tighten its grip.
Other Medical and Research News
Sarah Constantin does her dive on gas stoves, here are her conclusions:
Gas stove usage is not consistently associated with childhood asthma or respiratory disease generally; there are numerous negative results and most of the positive results are confounded.
Even those studies that found an effect had fairly small effect sizes (almost all ORs under 2.0).
High nitrogen dioxide is associated with respiratory disease. Using a gas stove without ventilation, or spending a lot of time cooking on a gas stove, might be a risk factor for respiratory disease even if gas stoves overall are not.
Induction stoves may even have health downsides relative to gas stoves— they’re associated with higher rates of birth defects in China.
She also notes that the paper that got the whole week of internet hoopla started not only contained no new data and did fairly represent the data that existed, it also was clearly a hit job motivated by environmental concerns.
New paper says: Consolidated ‘health systems’ of doctors and hospitals slightly raise quality of care and patient satisfaction. They raise costs quite a lot. In most places customer satisfaction would take into account the price. Alas, this is health care.
Saloni Dattani roundup of events since December. Cancer deaths are down 27% after controlling for age. Modern hospitals reduce infant mortality. Intelligence correlates with openness. Major droughts increase religious observance. Cash incentives up front are cost-effective at reducing air pollution on Indian farms, saving lives for less than $5,000 – new EA cause area? Also where to find birds and an exploration of the gender pay gap.
A fentanyl vaccine has been developed. Great news. We still have to wait for the human clinical trial results, so any number of things could still go wrong. If they don’t, we will have a vaccine that, if boosted every few months, means fentanyl won’t get you high and also you won’t overdose, with no substantial side effects.
The tricky question is: What do we then do with it?
The hope is that this will become available freely to those who want it, and many addicts or those at risk accept the offer. A lot less of those people die. Those who cut other drugs with fentanyl get caught by the vaccinated noticing they are not getting sufficiently high, so that practice mostly stops, protecting others as well.
Will there be much voluntary uptake? My guess is there would be, if the vaccine was offered freely and anonymously. Few people want to be hooked on fentanyl, and those who want to take other illegal drugs don’t want to die if someone spikes their supply.
The bigger worry is if this tool is available, to what extent will it not stay voluntary? Will we mandate it for those who overdose? Who seek treatment? Who are in prison? As a condition of welfare, custody or a job? Or parole? Who are at-risk youth? Everyone? What comes next if we do that? What does all this do to the public’s relationship to vaccines, public health and government mandates?
We already mandate people stay on various medication, or else, in various ways. Even if the government stays out of such matters, even if it is illegal to require the vaccine for things like employment, there will doubtless be a lot of ‘or else’ going around. Many historical parallels suggest this could quickly get ugly.
Despite all that, we must remember: This development is still great news.
FDA announces new action standards for food containing… lead? They expect this to cut lead in food by 24%-27% (what a precise window) but… was this a problem?
We have a new entry in ‘I don’t really know what I was expecting (or smoking.)’

“Did we know there would continue to be an illegal market even as we rolled out and grew a legal market, yes,” Krueger said. “But I don’t think that we saw anything like this happening in the other states where there was almost an organized come on in and just start opening all these stores.”
When I walk around NYC now I constantly see ‘smoke shops’ and ‘dispensaries.’
It turns out that
People like their drugs.
People like the illegal versions better.
Probably because they’re cheaper and higher quality.
Legalization made the law against technically illegal sales hard to enforce.
If you don’t enforce the law against the better option, people will take it.
I am shocked, shocked. The real question is why this didn’t happen elsewhere. My guess is some combination of too many frictions going the legal route, and most the rule that the legal weed has to come from New York when we all know the good stuff comes from California, or at least not from New York.
I think, as a corollary to never interrupt your enemy while they’re in the process of making a mistake, we may adopt never interrupt someone when they’re doing something you want, even for the wrong reason. Or, at least, maybe “taxpayer dollars” is the good-sounding excuse and they actually want to ban GoF for its world-ending powers and just can’t say that directly.
Don’t take this too far though; calling out bullshit may still be valuable even if it’s bullshit that temporarily supports “your side”: ideally doing so helps raise the sanity waterline overall, and more cynically, bullshit may support your opponents tomorrow and you’ll be more credible calling it bullshit then if you also do so today.
But in this exact case, banning GoF seems good and also not using taxpayer dollars on negative-EV things seems good, so these Republicans are just correct this time.
This is true, too. Perhaps we can refine it as never interrupt someone when they’re doing something you want, unless their reasons would incur other damage—this lets us ban GoF while only caring about taxpayer dollars (true but not the main reason) while avoiding banning GoF for, say, pwning the Democrats (bad if we start doing more things to pwn the Democrats).
If the republicans are bringing out the accusations of exploited taxpayers, then you know they’re serious.
(disclaimer: this doesn’t actually tell you how serious they are, the only way to track the seriousness of anything related to congress is to follow the money).
The reason for moving to single doses of covid vaccines are simple. They are the same as the reason we have single doses of flu vaccines. EVERYONE has immune memory except babies, be it from infection or a previous vaccine. Once you have that established memory, doubling up additional doses doesn’t accomplish much.
The proposed legislation regarding gain-of-function research is meaninglessly vague and pointless.
Additionally, seriously, stay the hell away from Ebright and everyone and everything he amplifies. He is a deeply unserious crank who constantly points at other cranks liars and who I am yet to see say anything sane or interesting.