I’ve always at least somewhat tried to model these posts after the pure joy of America’s only true newsletter, Matt Levine’s Money Stuff. This week I finally got around to listening to Matt do this amazing podcast about the philosophical side of what he does, which I highly recommend. Covering Covid means that the subject matter is always, at its core, a combination of people dying and a portrait of civilizational collapse. The whole situation is usually rather dismaying. It is likely to remain rather dismaying permanently.
Thus it is not the ideal place to find delight in one’s understanding. Nor is writing up the rise of monkeypox or our national failure to be able to keep even normal baby formula in stock while every other country on Earth has no such issue and most of them are happy to sell formula to us, which has now extended to our family being unable to find any normal brands on Amazon or other online sources, forcing us to buy organic formula instead, which was fortunately available as a still-legal form of price gouging.
I am thus excited to once again see the weekly posts decreasing in size as the amount of Covid news decreases. If this continues, soon these posts will be quick to put out, and some time after that perhaps they can stop being weekly.
I’m hoping to pivot away from short term developments and towards more longer term, less speed premium explorations of how the world works, in places that can lead to more generally useful insight and more delight, although still with a lot of silent screaming about the ways in which things are terrible.
One key is that I like to think of finding out things are terrible, whenever I can, as good news and a source of delight. As long as we know roughly how bad things are already, identifying the sources and finding them to be crazy unnecessary idiocy is often good news. It means things can more easily be fixed.
There were some new Long Covid claims this week I felt compelled to respond to, but there isn’t a big update to make as a result.
Executive Summary
Covid-19 still exists and BA.4/5 have substantial immune escape.
Thus I keep doing these posts every week.
Ideally they keep slowly getting shorter.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 700,000 cases (+17%) and 2,100 deaths (+5%)
Results: 643k cases (+7%) and 2,337 deaths (+17%).
Prediction for next week: 700,000 cases (+9%) and 2,725 deaths (+15%).
Note that Florida has been adjusted to account for its reporting schedule. It still saw a large increase. Also Vermont failed to report so I gave it last week’s number.
The surprise was an active decline in cases in the Midwest and East, without any holiday to explain the change. It seems odd for things to reverse in this way, but the prediction has to hedge its bets.
For deaths, cases have been climbing for a while so now that we see the numbers trending up and we’ve wound through our backlogs it makes sense for the number to keep rising for a it.
Deaths
Cases
One could explain the different trajectories using weather or one could say that some places have already peaked because different variants spread in different places at different speeds and times, or both. It could also be some sort of reporting artifact, I’m not yet sure what to make of it.
The Never-Ending Pandemic
Here we go again with slight variations edition: A prediction that Covid will not only stick around, but ‘infect most people several times a year.’
The central problem is that the coronavirus has become more adept at reinfecting people. Already, those infected with the first Omicron variant are reporting second infections with the newer versions of the variant — BA.2 or BA2.12.1 in the United States, or BA.4 and BA.5 in South Africa.
Those people may go on to have third or fourth infections, even within this year, researchers said in interviews. And some small fraction may have symptoms that persist for months or years, a condition known as long Covid.
“It seems likely to me that that’s going to sort of be a long-term pattern,” said Juliet Pulliam, an epidemiologist at Stellenbosch University in South Africa…
“If we manage it the way that we manage it now, then most people will get infected with it at least a couple of times a year,” said Kristian Andersen, a virologist at the Scripps Research Institute in San Diego. “I would be very surprised if that’s not how it’s going to play out.”
The math on this claim is interesting. If ‘most’ people are getting Covid at least a couple times a year, I would assume that means at least an average of two infections per person per year, so in a nation of 330 million that is almost 2 million cases per day on a permanent basis. Each day, 0.55% of the population would have to be infected.
As a comparison point, there were just short of 750k confirmed and recorded infections per day at the height of the Omicron wave, a pace that was sustained for roughly three weeks. Most infections are not confirmed and recorded, especially asymptomatic ones, so that doesn’t render a steady state of 2 million per day impossible exactly if the virus continues to mutate at lightning speed, but it does not seem like where one would set the betting line.
The next question is whether or not something like a soft version of this scenario should bother us. It may sound bad to get Covid-19 several times a year, and obviously it is far worse than never getting Covid-19 at all, but is this actually a problem?
If one has the model that each infection is an additional independent chance for bad things to happen, then it is very bad. If you think those bad things prominently include a big risk for Long Covid, it’s even worse.
Note that even if all that was true I would once again (to repeat the argument) strongly urge almost everyone (some people are immunocompromised or in some other unique circumstance where it’s less clear) not to go into permanent midnight mode and hide away from the world. You can protect yourself by doing so, but what are you protecting yourself for? Again, this would be a permanent condition of life. So the only option would be not to live it. Life must go on. If there was a condition with a side effect of having to do Covid prevention all the time, you’d try very hard to avoid it.
I can already hear some of you saying that you’re introverts who are perfectly happy to never leave the house. I do agree that if this was already something you were happy to do, this would be a marginal additional reason to do that, or to do it more. I would also say that I think most such people were always making a large mistake.
Or, more bluntly:
However, if the infections do come fast and furious, there’s also the more likely scenario where all of this is good. If everyone is getting infected every few months, then that is enough time to still be well protected from severe disease and death based on the last time you got infected. Even more than now, most cases will be fully asymptomatic and most other cases annoying. Yes, there will be ‘another flu’ running around of some average severity, and that will make life permanently worse. But the default will not feel like getting infected multiple times a year, certainly not with anything serious.
My model of Long Covid continues to think that if you get a reinfection that doesn’t produce symptoms, the chance of this causing Long Covid is miniscule – if getting infected more often means total severity goes down, then total Long Covid would likely decline as well.
If we do find ourselves in the lots-of-infections scenario, and somehow we also end up in the and-the-infections-are-much-worse-than-all-that version of that scenario, then what could we do about it?
Barring further technological and scientific developments, nothing. None of our options for making this not happen are worth their costs.
With proper pandemic funding for new development, we can change that. Nasal vaccines are highly physically possible and could be developed, which would halt the spread and end the cycle. Or we could use a variant-proof neutralizing antibody – recently we discovered another one.
Alas, we are unwilling at this time to fund them.
The bottom line remains that we’ve decided not to care. There are many advantages to that in terms of not doing crazy prevention that is worse than the disease, but it means we are not doing the most basic common sense things we need to be doing. That’s what it means when Congress funds literal nothing.
FDA Delenda Est vs. Vaccines
This is, as far as I can tell, real.
Let this sink in. The FDA wants to change the formulations of the vaccines because they are worried not doing so would ‘befuddle’ people.
I happen to think the exact opposite. Different people like different things. Making this seem more like a choice seems likely to be actively good. I would not, however, be so bold as to change the formulations of the vaccines to try and play mind games with the public.
CDC vs. Paxlovid Rebound
Here are the CDC guidelines for anyone who gets Covid-19, takes Paxlovid, and then experiences a rebound.
The basic logic of this document goes something like this:
If you get a rebound ‘there is currently no evidence’ you need treatment.
We don’t know if such people can transmit or how likely it is.
So sure, why not, isolate for another 5+5 days.
And no, we don’t ask for a negative test, why do you ask?
That last one is a continued source of frustration, but in these circumstances it’s less stupid and either way it’s not going to change. Given that, I don’t see a way the CDC could have issued better guidelines.
This harkens back to the thread last time when someone who was worried there might be Paxlovid rebound worried about whether to pre-emptively keep isolating, which was rather a lot over the top and is definitely not necessary. Doing it once you actually get a rebound case however seems reasonable.
Also test-to-treat sites are being opened to help with Paxlovid distribution. Not all that many, but it’s at least something.
Long Covid Yet Again, Sigh
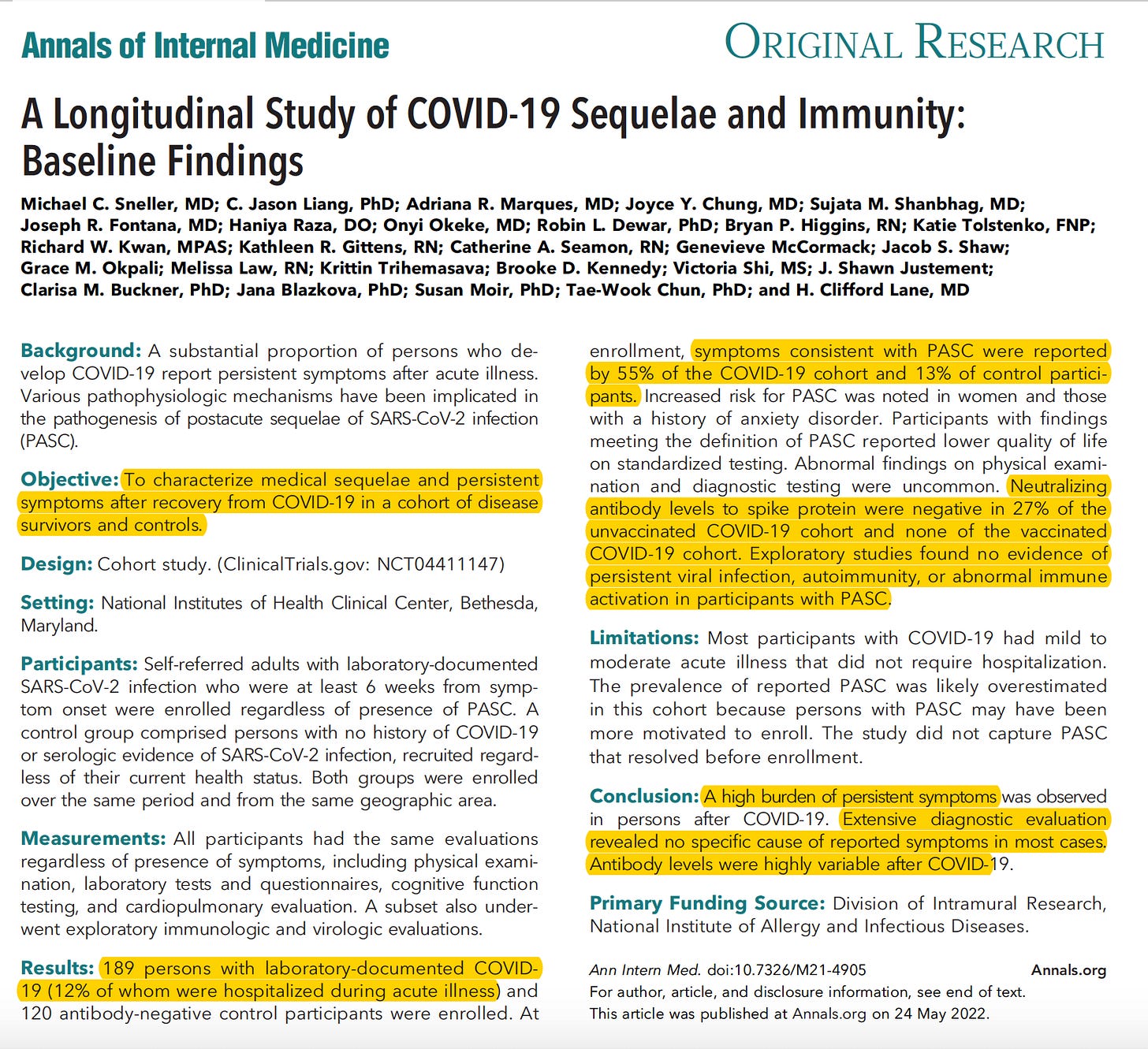
Enough people mentioned it that I too hate to mention it. I was sent this Washington Post article about the new Nature paper claiming that vaccination was not protective against Long Covid. The paper is here.
Paper did not move me substantially from what I said in The Long Long Covid Post.
Explaining why would mostly be a rehash of that post.
Here’s the bullet point version.
This only counts cases not infections, which understates vaccine effectiveness.
Study pre-dates Omicron.
Vaccination did reduce risk for all death in the Long Covid period by a third.
Vaccination was also protective against problems in the lungs.
Vaccination only reduced claims of other symptoms by 15%.
One interpretation of this is that Long Covid is real, it is everywhere, it is not much reduced by vaccination, and thus it also must not care much about severity of the infection.
Another interpretation of this is that those who say they suffer from Long Covid are mostly not suffering from Long Covid.
Instead, this would be a mix of:
A: Those who get Covid being less healthy, those whose Covid is detected being less healthy, and controls not fully handling this.
And B: Those whose Covid is detected being more likely to report things that they believe are wrong with them both because it is in their nature and because they are more likely to associate the issues with Covid and thus report them.
I do not consider this strong evidence against the model that I presented in The Long Long Covid Post. It’s mostly duplicative.
I have intentionally been avoiding discussing news on Long Covid that didn’t adjust my priors, including news that supports my priors to avoid the resulting bias. Thus, most of the time, when there are absurd claims like ‘one in five people are suffering from Long Covid’ I usually neither point out the claim nor link to those who point out the absurdity of the claim.
I don’t know any way to describe this except you can’t do that, you can’t do any of that, you people are cheating, you know you are cheating and you’re doing it anyway.
What the CDC did in the claim in question is deeply, deeply alarmist and irresponsible.
Also, when one reads the report: Matched controls? What are matched controls?
Control patients (1,640,776) had a visit in the same month as the matched case-patient (control index encounter) and did not receive a COVID-19 diagnosis or a positive SARS-CoV-2 test result during the observation period. Controls were matched 5:1 with case-patients. All patients included in the analysis were required to have at least one encounter in their EHR during the year preceding and the year after the index encounter.
I mean, here’s what they say among other things about ‘limitations.’
Second, the incidence of new conditions after an acute COVID-19 infection might be biased toward a population that is seeking care, either as a follow-up to a previous complaint (including COVID-19) or for another medical complaint, which might result in a “sicker” control group leading to underestimation of observed risk.
I have a rather endless list of Long Covid claims that I could, in theory, spend the next week or three checking out in detail. I am going to go ahead and continue not doing this.
I do sympathize with the people trying to study this and doing their best to untangle the puzzle as opposed to trying to show how awful things are and scare people. The nature of the problem makes the question extremely hard to study if you’re interested in getting the real answer. The ways to actually, fully get a reliably correct answer here that I can come up with seem prohibitively some mix of expensive and otherwise (for ‘ethical’ reasons, sometimes even for actual ethical reasons) impossible.
This week there was also this prospective small study for what it’s worth, which I will offer without comment.
Going forward, my policy will continue to be:
If something involving Long Covid changes my model I’ll discuss it.
If something doesn’t change my model much, I’ll do my best to skip it.
If you want to hire me to look at stuff anyway, you can pay my hourly.
I guess. It’s your money.
I mean, my model says you totally, totally should not hire me to do this.
BA 1 2 3 4 5
Europe has upgraded BA.4 and BA.5 to variants of interest. That seems right.
This thread gives us details on the bad news. BA.4 and BA.5 indeed have meaningful additional escape properties (link to paper), but the escape is not total, and the escape from BA.1-breakthrough-elicited antibodies is not as bad.
Prevention and Prevention Prevention Prevention
I forgot to mention this last week but North Korea went into full lockdown, on top of its permanent other full lockdown. If there’s one country that could pull off actually keeping the virus out this way, North Korea is probably it, so I’m not even completely convinced the decision is wrong.
An estimate that good ventilation reduces Covid transmission by ~80%.
An important safety tip.

In Other News
A correction in the New York Times.
Original:
Correction:
Yeah. Whoops.
Think of the Children (non-Covid Edition)
Tragedy struck this week in the form of a school shooting in Texas.
As a result, there was another round of gun control talk, and another round of terrifying our nation’s children. I don’t have anything to contribute here on gun control that you haven’t already heard many times before.
Instead, I mention this because of the other things people are talking about doing. What we need to avoid doing is compounding the tragedy of school shootings by doing serious damage to all of the children in school in the whole country.
Having children constantly walk through metal detectors, or removing doors from buildings, or having teachers carrying guns, or treating any child who does anything weird or makes their fingers into a fake weapon as a potential serial killer, or most importantly doing traumatic live shooter drills, are profoundly terrible policies that impose huge costs on our children’s lived experiences. They turn school and life in general into something experienced as a generally unsafe environment.
All of that really is incredibly bad. It bears keeping in mind the magnitude of the problem:
The database documents when a gun is brandished, a gun is fired, or a bullet hits K-12 school property for any reason, regardless of the number of victims, time of day, or day of week. There have been 1,322 individual shootings since the 1970s, resulting in 426 deaths and 1,225 injuries.
That’s less than 10 deaths and less than 50 injuries per year for the entire country, out of roughly 50 million students.
Would preventing that be worth a decade of going through metal detectors and periodically being traumatized by pretending you were being hunted by a killer and teach them to view the world through the lens of firearms even if it fully worked? I know if I was choosing for my own children I would answer an emphatic no.
And there’s no reason I can see to think such measures are all that effective. There’s even reason to suspect that creating a culture in which children are taught that school shootings are far more common than they are, that they are expected behavior, could be a large contributor to why we have so many such shootings. The idea to do it has to come from somewhere.
One can also point out what happened with the police failing to stop the shooter. It’s one (already crazy) thing to have a bunch of people with guns hanging around your kids constantly in order to stop a one in a million risk. It’s another thing to have people with guns hanging around your kids who when the time comes if anything actively prevent people from stopping the one in a million risk.
Those who buy a little temporary security often do not get what they paid for.
This all echoes ‘stranger danger’ and our general insanity to not let kids do things like ‘play outside on their own for ten minutes’ without calling social services. Toddlers in Japan go on errands on Netflix, and that is extreme but very much The Way. Instead, we refuse to let children live life.
It all also echoes, of course, Covid-19, both what we did as adults but especially what we did to kids. Kids were always in almost zero danger yet we sometimes still force them to mask and even shut their schools down and not let them see their friends.
The things that we do ‘about’ school shootings, and might do more of now, are more of the same, only with even less justification.
In Other News
I feature in this Matthew Yglesias mailbag. He also wrote this piece about Sam Bankman-Fried and effective altruism.
ㅤ
This seems backward. The first quote implies the FDA wants to avoid changing the formulations.
I frequently encounter people who see vaccination as a cure-all that protects them from getting brain damage or permanent fatigue from COVID, and engage in risky behavior as a result. In reality, this n of 30,000 study by the VA strongly indicates that vaccines do virtually nothing to protect against brain damage or permanent fatigue. And considering the mere existence of the Omicron outbreak, they probably don’t do much to protect against infection either.
This worries me greatly, since many of these people are in really important positions, and I wouldn’t want to live in a world where they are brain damaged, or have to retire early due to permanent chronic fatigue. Especially if treatment availability or herd immunity are <1 month away.
Staying inside for another month or two has its own long-term hazards which are also very grave, like getting addicted to a malevolent social media app, which is also worth significant consideration. But it should be considered against the current wave, which might actually be avoidable (unlike omicron), due to the stronger herd immunity that everyone got from BA1 in January.
I am somewhat skeptical of the “1-month away” phrasing, since I have heard it every month for the last two years. I worry that I’m rounding you off to a position you don’t actually hold (in which you are perennially advocating for caution, but claiming a new development is just around the corner). Rather than assume, I think it would behoove me to ask about your past behavior: During what times of the past year or so did you have advocated for only very limited covid avoidance strategies (e.g. not meeting with people who are currently displaying symptoms of covid, preferring better ventilated or outdoor venues for large events), but encouraged or at least not discouraged behavior that carries some risk (going to events with many people, wearing a mask only if you feel like it, etc.)?
I’m a dumbass who didn’t know about p100 masks until a post on lesswrong told me about them, about two months ago. I also didn’t start quarantining seriously until late january, when it was far too late (no known long-covid symptoms in my case). I even used surgical masks throughout 2020 and most of 2021, because I didn’t know better. I did all these incorrect things, even though I knew that Covid is a brain virus, since summer 2020, but I didn’t have any concrete data about the brain damage and disability whereas now I have a pretty good general idea.
I didn’t know how easy it was to avoid catching the virus and how worthwhile it is to do so.
Also, we’ve never, ever been anywhere near this close to herd immunity, due to omicron probably infecting everyone everywhere in January. And since the current variants are stalling, it seems to me like they’re hitting a wall of that herd immunity as each variant runs out of high-risk people to spread to. So the expected cost-benefit ration is higher than ever before of being less-brain-damaged-than-par.