We finally have a date. On May 11, the official Covid Emergency ends. The actual emergency is, of course, long over, but for technical reasons the official change will have to wait a bit.
A related question is when it stops making sense to continue writing weekly Covid posts. My basic plan for a while has been ‘when there stops being content for them’ and somehow I still end up with a bunch of content every week. That does not mean this is the right format for that content, or that this is the right content to be creating.
I will continue to think more about this, and have not made a decision yet.
The other news is that we finally have a reformulation of all shots of the Covid vaccine… to the version we approved for boosters that is already out of date. We will likely never have a properly up to date Covid vaccine again. Oh well.
Executive Summary
Covid emergency to end on May 11, 2023.
Vaccine formulations all to be updated to bivalent composition.
Other news will be covered in roundups soon.
Let’s run the numbers.
The Numbers
Predictions
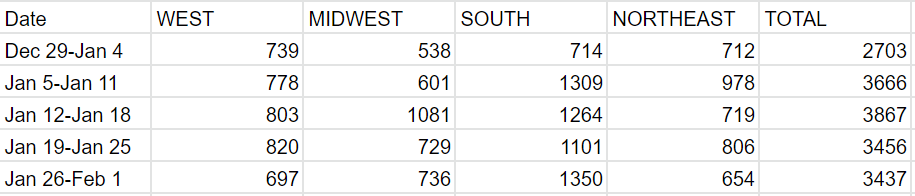
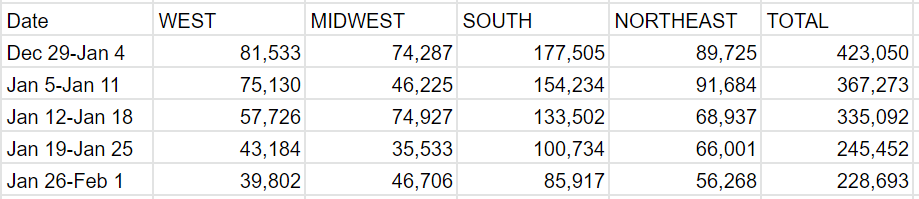
Predictions from Last Week: 223k cases (-10%) and 3,300 deaths (-4%)
Results: 229k cases (-7%) and 3,437 deaths (-1%).
Predictions for Next Week: 210k cases (-8%) and 3,150 deaths (-8%).
Everything seems right back on schedule. I see no reason this shouldn’t continue.
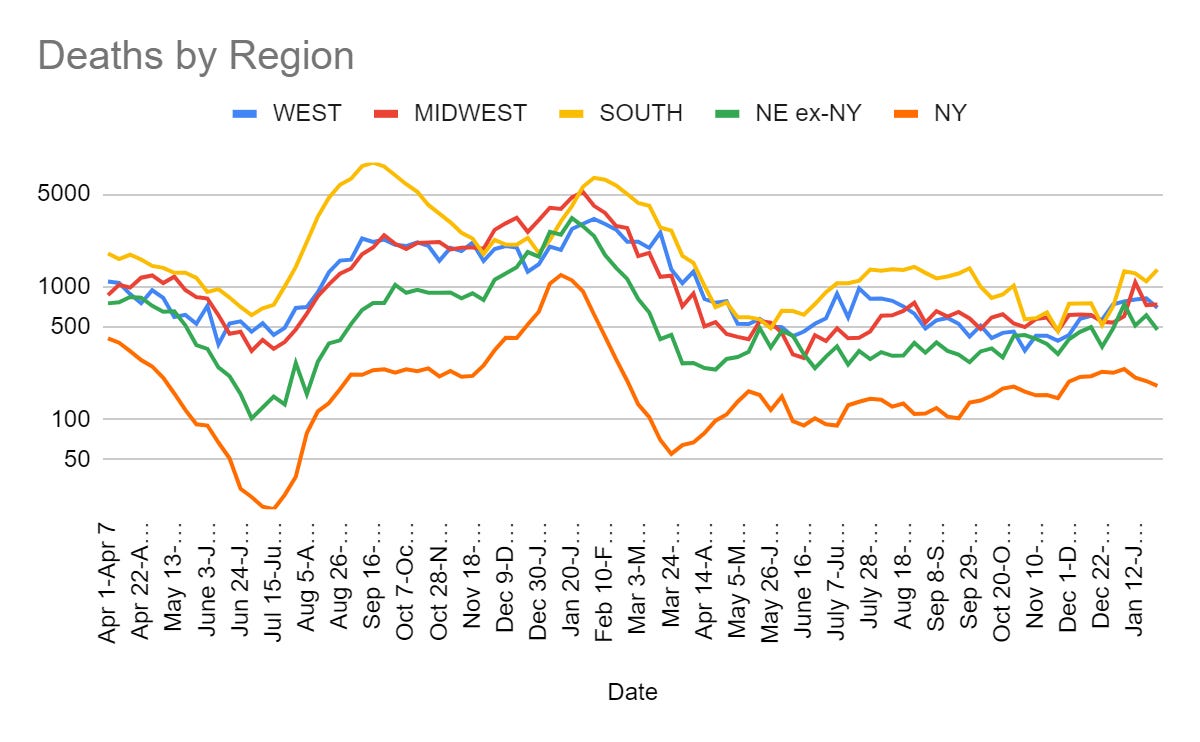
Deaths
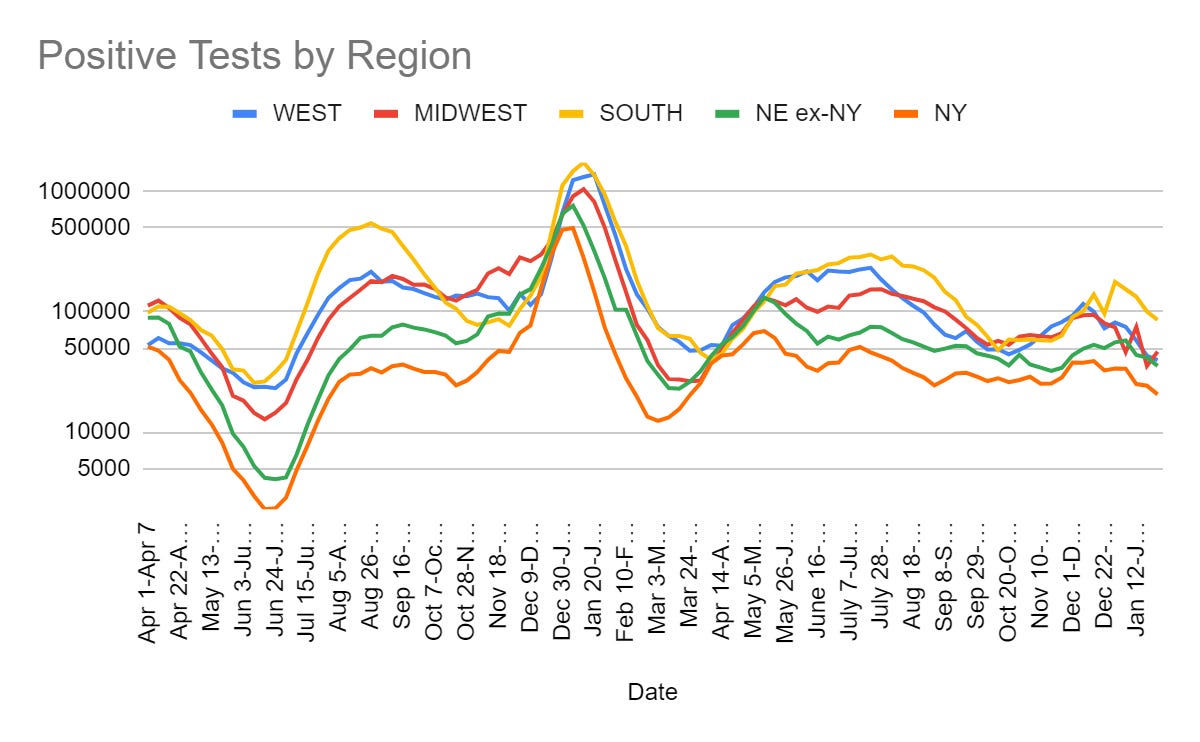
Cases
Physical World Modeling
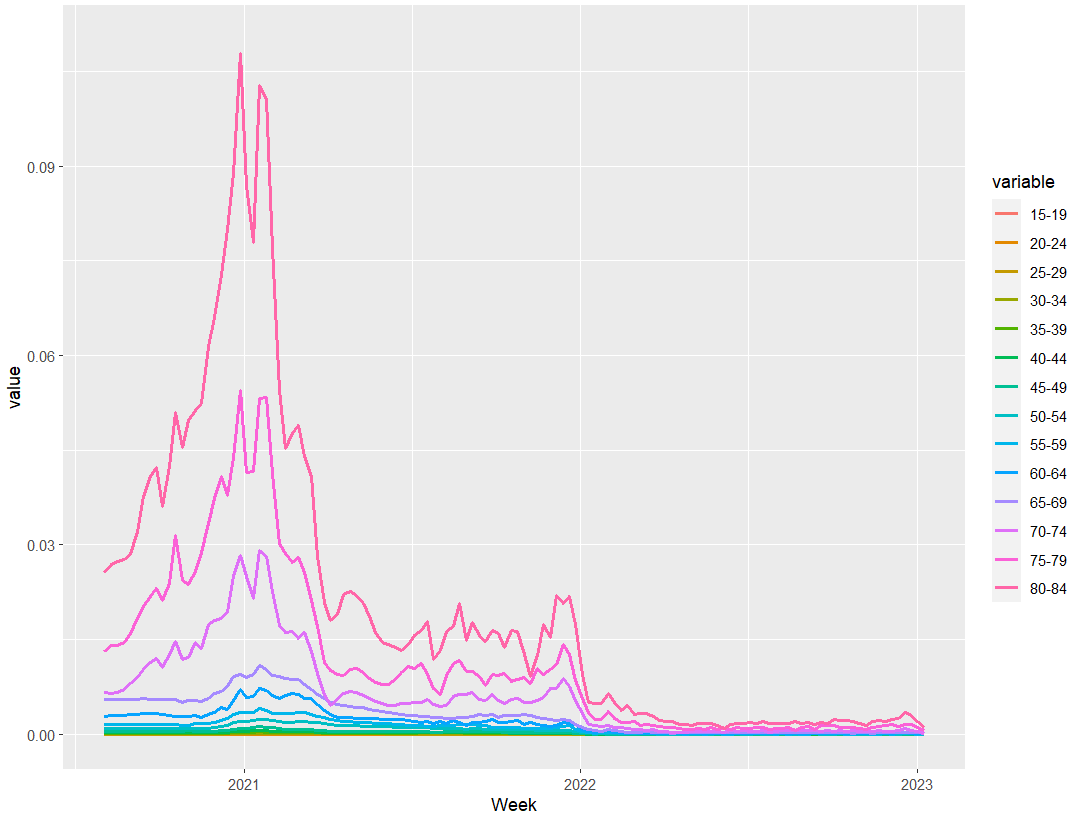
Covid death rates by age, over time, on a log scale, as Covid deaths with a two-week lag divided by reported Covid cases. Cases are vastly undercounted, far more than deaths could possibly be, so the CFR here remains much higher than the true IFR.

I think some of the wonkiness here is that two weeks is a little bit short in terms of lag.
See the sharp drop with Omicron’s arrival.
For reference, here’s the linear scale.
Most Long Covid studies continue to be terrible and tell us nothing. This one was especially terrible.
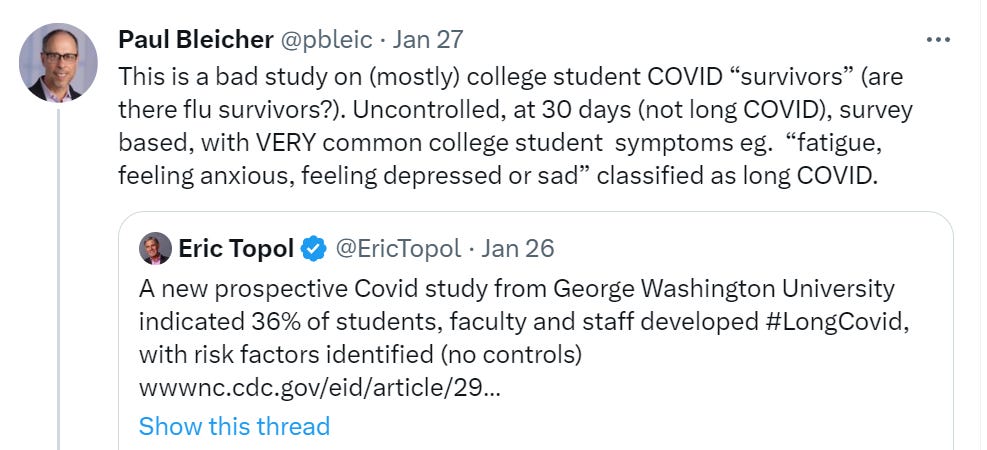
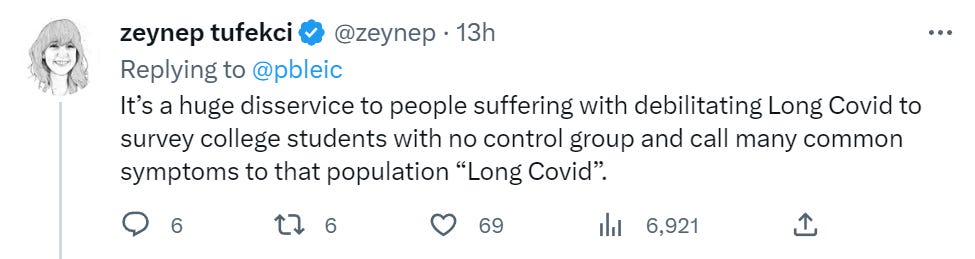
Zeynep thread on how people use snippets, selective quotes and screenshots to misrepresent scientific findings and scare people, if you need another of those. She is performing a public service here, yet I grow weary. Chise thread covers the meeting.
Molnupiravir conclusively caused Covid-19 mutations in the wild. Kind of wild that we allowed people to use it. We should stop allowing that.
Bloom Labs thread on predicting future mutations and their impacts.
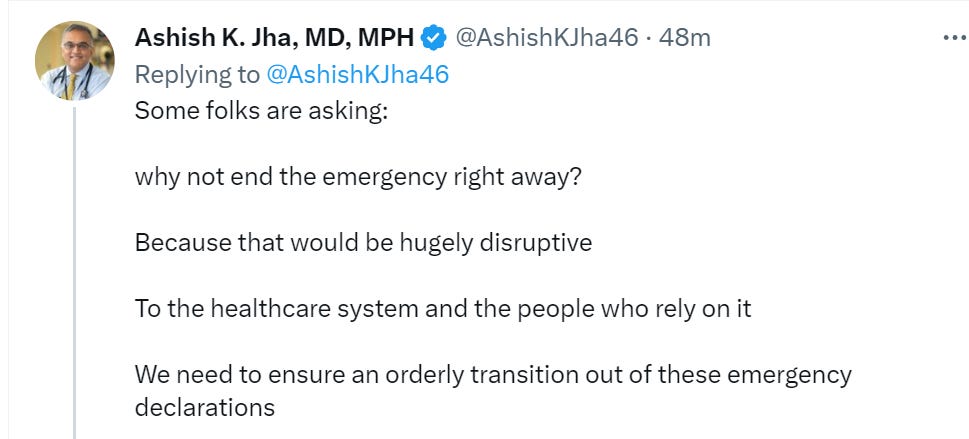
The Emergency Will End on May 11
That is quite a long time for there to be an emergency after you know you can safely end the emergency. What’s up with that?
To public health professionals, the difference between an emergency and a non-emergency is what they can get declared an emergency. I mean, I get it. Consider how many people go to the Emergency Room. If people are getting sick and dying, that is at least somewhat of an emergency. How could you dare withhold any care based on my ability to pay? Or make me pay for it, even if I could? The planetary death rate holds steady at 100%. Where does it end or begin?
Either way, I am happy that this ‘emergency’ is finally coming to an end, even with a crazy long delay. The other emergencies will continue until morale improves – there are currently 42 in effect, a majority of the emergencies ever declared.
Especially good news is that the FDA clearance of Covid vaccines and treatments ‘won’t slow with end of the public health emergency.’
Given we already know the speed at which the FDA has been approving things – faster than usual while still slow enough to kill a lot of people and ensure we never have the vaccine or treatments in a state that keeps up with the virus or impacts a wave before it happens – it is good that it is not about to get even slower.
It is still worth asking, if the FDA cannot use a literal health emergency as a way to speed up the process, what would let them speed up the process to the point where it had any chance of working?
Meanwhile, the current system is working as designed I suppose:
FDA advisory committee votes 21-0 to update all Covid-19 vaccines in circulation to the bivalent vaccine for original strain combined with BA.4/BA.5. Better to do this than do nothing, I guess. Went perfectly. That goes both ways. This is the timeframe for implementation when everything goes perfectly. Very large will-always-be-far-behind vibes.
Some Weekend Reading has a full breakdown, if you’re interested in that.
It seems like this was an awful lot of machinery to crank up just to come to the only sensible conclusion? Even though, as we’ve previously noted on this Crummy Little Blog That Nobody Reads, they’ve previously promised to review COVID-19 vaccine composition quickly like they already do with flu vaccines.
My personal guess is that a lot of this is due to 2 reasons:
The natural extreme caution of medical regulatory bodies, where they want to be sure they’re not hurting anybody, and probably doing some good.
The superstitious fear of COVID-19 vaccinations among about 1⁄4 of the US population. They again want to be sure they can point to hard evidence for their decisions, since being hauled in front of a Congressional committee headed by intellectual giants like Marjorie Taylor Green would drive anybody into detailed, defensive documentation.
In other words, yes, the FDA flat out broke its promises on this and we have no reason to expect this to change going forward.
In Other Covid News
Marjorie Taylor Greene appointed to House Covid Committee. This is quite the bad sign for how the Republican House is going to be going about its business. I do not think it is ‘dangerous for our national security’ unless essentially everything is. Our legislative system needs to be able to survive having a wacko on the wrong investigative committee, or we have far bigger problems.
WHO is worried we might not be worried about Covid.

Why would we want to ‘maintain the global and national focus’ on Covid-19?

There is of course still a need to continue developing vaccines, diagnostics and therapeutics, the same as with every other disease.
China


Remember
Private for-profit nursing homes instituted less Covid-19 restrictions than not-for-profit nursing homes. This caused more Covid-19 deaths but less other deaths and less deaths overall. This makes perfect sense given the incentives involved.
A simple story of the good-science to anti-vax-community pipeline. My summary:
Demand for alternative-explanation Covid content is off the charts.
This is stuff like Ivermectin. All part of a pattern language.
When content producers try such content, they get crazy high engagement.
Content producers really like crazy high engagement. Good for business.
To keep and grow that engagement, you have to keep raising the stakes.
Anti-vax community offers you big bucks and engagement.
Even if you want to turn back, you can’t, because you’re blacklisted.
Might as well keep going and cash in.
Notice: This is extremely similar to what happens in broader discourse.
The more general case:
Power demands adherence to a single Narrative and set of Truths.
Power casts out anyone who is seen opposing that Narrative and set of Truths.
This casts many in opposition.
This creates an attractor for an alternative Narrative and set of Truths.
This second attractor, alas, mainly optimizes for opposition to the original Narrative and appeal to those who want to stand in opposition.
These beliefs contain a lot of Obvious Nonsense, optimized to be as awful as possible. Reversed stupidity is not intelligence.
Anyone cut off from the Narrative risks being drawn into the second attractor.
The second attractor often also incorporates some true and useful information, which then becomes too toxic to touch, drawing those who notice that these true things are true into the second attractor.
Thus, over time, a lot of people who would otherwise have been reasonable end up with remarkably similar sets of disapproved beliefs, mostly unrelated to why they originally got alienated from Power and the Narrative.
The existence of one faction implies the other, in a Hegelian dialectic.
Also see Scott Alexander’s Kolomogorov Complicity and The Parable of the Lightning.
Trump ally preparing hit job on DeSantis by showing his old support for vaccination.

I continue to hope that things are not this far gone, and such efforts will mostly backfire. Yes, there are places and groups that do not take kindly to a politician having been pro-vaccination. Are they big enough, even within a Republican primary, to overcome the people who would not take kindly to a politician having been anti-vaccination, not merely anti-mandates?
Even considering that primary voters usually care about winning general elections, and one would presume that an actively anti-vaccination candidate would have a substantial handicap there?
I don’t know.
We are not the only ones who are choosing not to remember, see for example the UK.
I continue to be confused on whether the Republicans think that if the House passes a bill then it somehow becomes law?

As I understand the messaging, the idea is: ‘The city of Washington is suffering because we don’t force people to show up so they don’t spend money here. Our solution is to force people to show up here so they will spend money.’
What a great metaphor for government.
Other Medical and Research News
Small anecdata that says vegans are very likely to be iron deficient, among other issues. If you insist on going down this path, seems worth getting blood tests periodically to check.
UK Universities have been warned to stop training so many doctors.
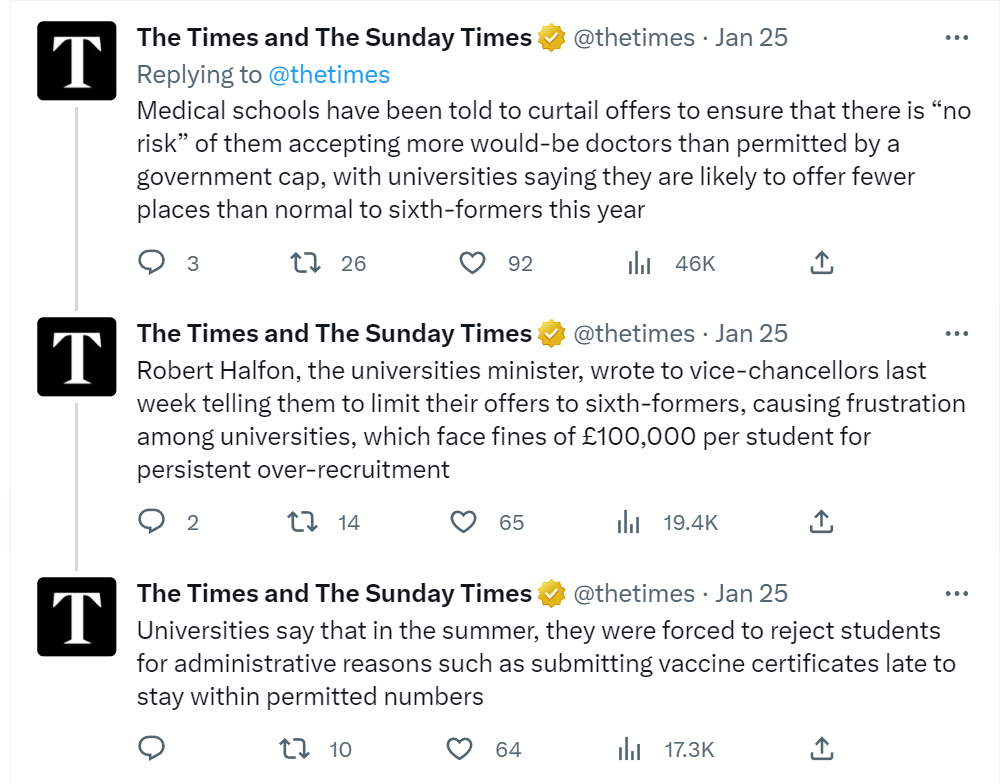
So there are schools that want to train doctors. There are qualified students who want to become doctors. There are patients who desperately need more doctors. Isn’t there someone you forgot to ask?
Why is our health system so overburdened? Why does everyone’s seem overburdened?
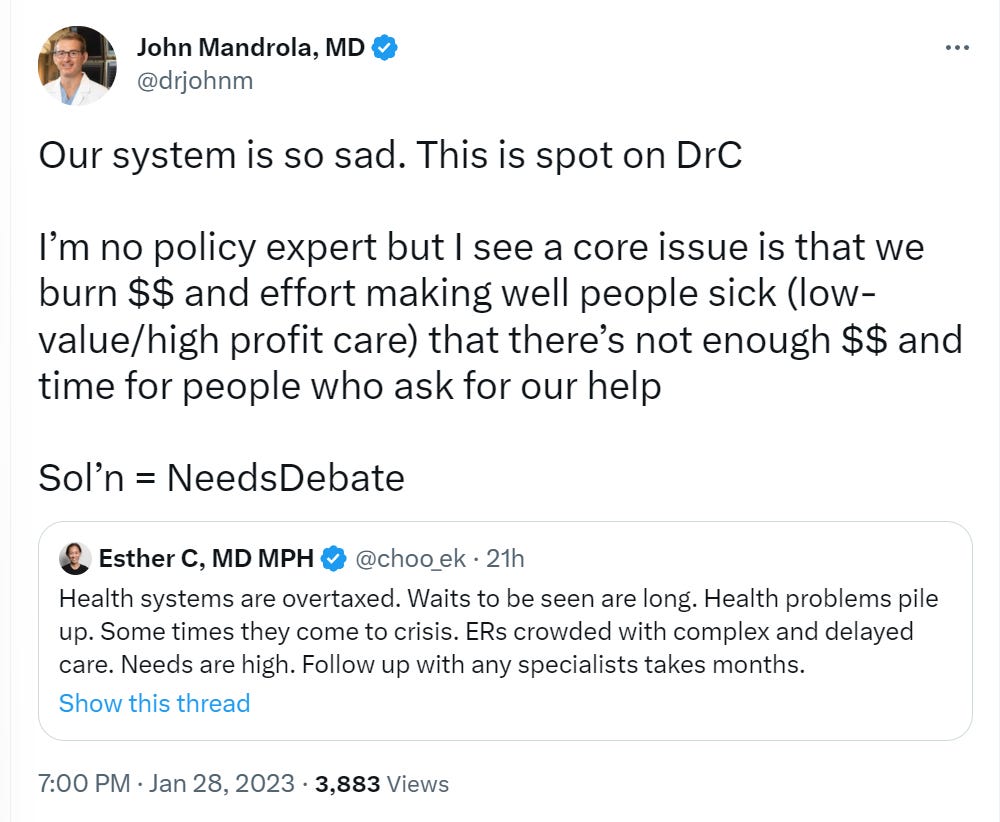
They are overburdened because we do not have a free market, those getting the services do not pay the price to provide the services, and do not allocate services by price.
You can quite reasonable say it is good that we do not do this. It certainly has some big disadvantages. It is still the fundamental cause of why we have a permanent mismatch between supply and demand.
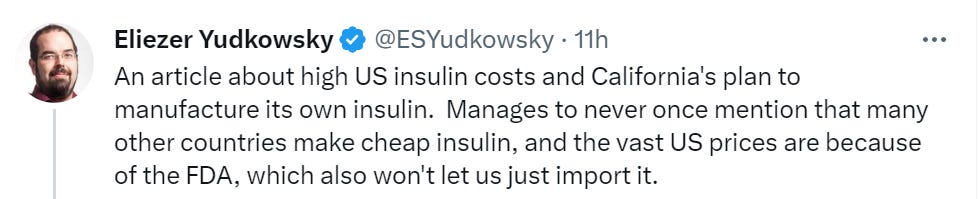
It is harder to say it is good that we don’t… allow people to purchase their life-saving medicine at a reasonable price, and are trying to solve the problem of a government ban on sane purchases with a government manufacturing plant.

Scott Gottlieb shares finding of secondary flu attack rate of 50% in 2021-22, versus 20% in prior seasons, speculates this was due to low exposure during pandemic. I am always surprised when the household attack rates come back so far under 50%.
Yes. This is exactly public health.
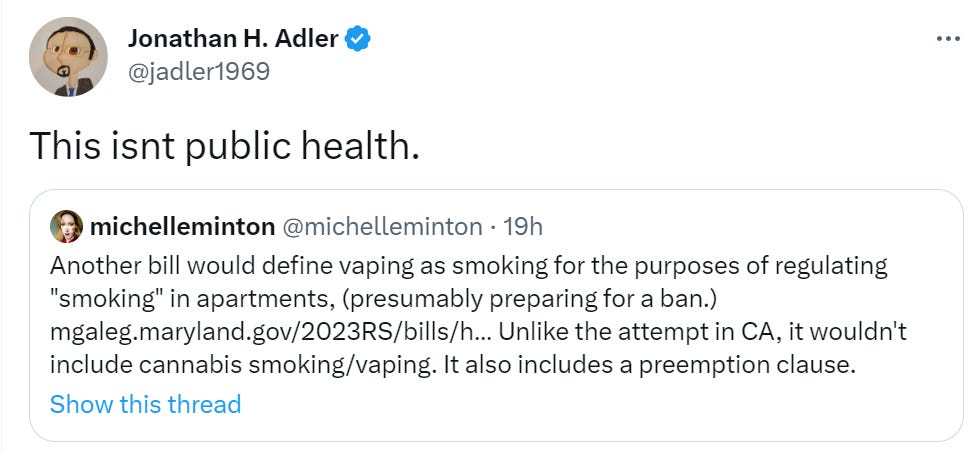
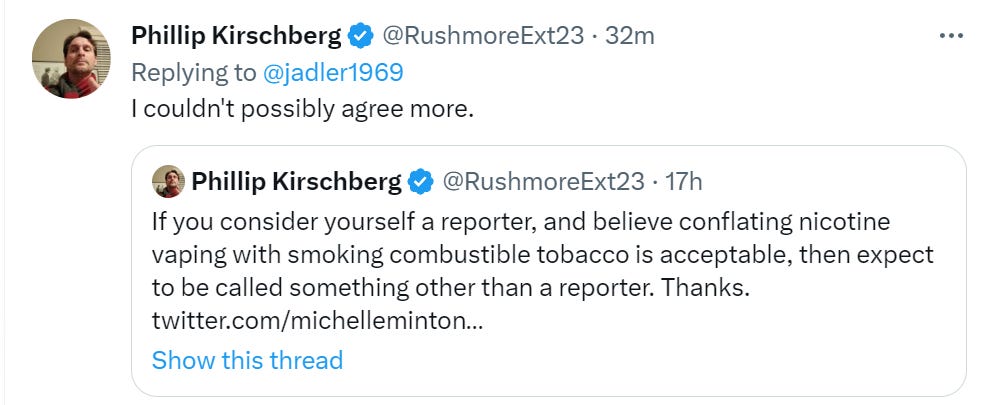
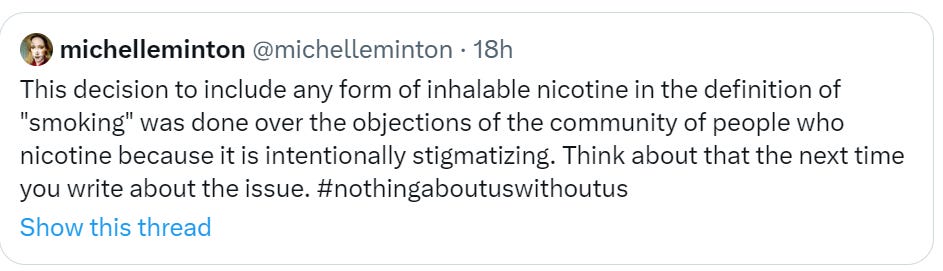
You are what you are in practice, not what you are in theory. You don’t to count the reasonable things and not the Obvious Nonsense. If public health keeps trying to ban vaping, if anything more aggressively than it bans smoking? That’s public health. If you do similar things in other areas? That too is public health.
FDA revises blood donation guidelines around MSM and sexual activity. My guess is this is a marginal improvement that does not address the core problems at all. We continue in practice to have some rather crazy rules around who we want donating blood, such as being sure to screen out anyone who might be doing it for the compensation. Heaven forbid.
Ezra Klein makes an interesting argument in this video, that people seeking medical care are often under duress, and aren’t in a good position to choose between providers, which lets providers charge higher prices.
I wonder if it would make sense to legally differentiate between “duress care” and “non-duress care”.
Has any health economist done a comparison between purely elective procedures like plastic surgery vs emergency procedures? I would imagine that plastic surgery (generally not covered by insurance) experiences less effect from government involvement in healthcare—so, when we look at the world of plastic surgery, does it look like a medical utopia? Is plastic surgery part of the general trend of the US having more expensive medical procedures than other countries? This article suggests that high US healthcare costs are a result of consolidation of hospitals & insurance companies, reducing competition. So maybe not?
What exactly is wrong with that?
Being at an investigative committee means she’s going to ask questions that more mainstream politicians would be uncomfortable asking.
Maybe she’s going to try to ask former Assistant Secretary Ford’s why he warned the AVG that their inquiry into the origins of COVID-19 and attempt to build a Bayesian model would “open a can of worms”? If the national security people thought that this kind of questioning was ‘dangerous for our national security’ they might still believe it to ‘dangerous for our national security’ for the same reasons.
The national security complex always thinks that putting people who ask inconvenient questions on investigative committees endangers national security. It’s also no surprise if the health establishment would hated a committee that asks Fauci real questions about how he lied about gain of function research. If Marjorie Taylor Greene pushes to go after Fauci for his gain of function-related purgery, that’s rightly worrisome from the perspective of the person you quoted.
Having her on an investigative committee is much better than a committee that’s about making policy. This is a job that she might actually be doing better than the average congressman while she’s likely worse at making policy.
In what universe is someone expliccitly committed to whipping up witch hunts and pushing conspiracy theories better equipped than a moron?
Generally, if you don’t expect there to be conspiracies going on, why would you need an investigative committee in the first place?
If the Church committee would have been made up by people who thought that the intelligence committee didn’t conspire to violate the law, it likely wouldn’t have been much use.
On February 1, Fauci mailed Auchincloss an email with an attachment called “Baric, Shi et al—Nature medicine—SARS Gain of function”. If I would be on the committee I would ask Auchincloss about what happened there and whether he thought that Fauci thought that the PDF described gain of function research. If Auchincloss says “yes”, than going after Fauci for purgery, for claiming in front of congress that it doesn’t, is a valid road to take.
Blatant purgery like that shouldn’t simply go unpunished. Putting people like her on the committee is a sign in the direction that the committee might actually have teeth and go for punishing it.
She’s certainly not a perfect being, but that’s not needed here.
You appear to have been taken in by liars and grifters. I suggest you reconsider your information sources.
My information source are the primary documents. The emails are public. Fauci’s testimony is public.
Is your crux whether or not Fauci sent the email with the “Baric, Shi et al—Nature medicine—SARS Gain of function” attachment? Is your crux about whether that was about the Baric and Shi paper from 2015? Is your crux about whether or not Fauci said under oath that this paper is not gain of functions research?
The policy you propose of don’t trust documents that the NHI released in response to FOI requests, seems like a stupid policy.