It was a quiet week. All the longer term news was as one would expect. That is good news.
The only surprise was that deaths jumped again while cases fell, rather than the other way around. On net, that too is good news.
If news remains this quiet for a while, I would be able to stop doing weekly Covid updates. Even more good news.
Executive Summary
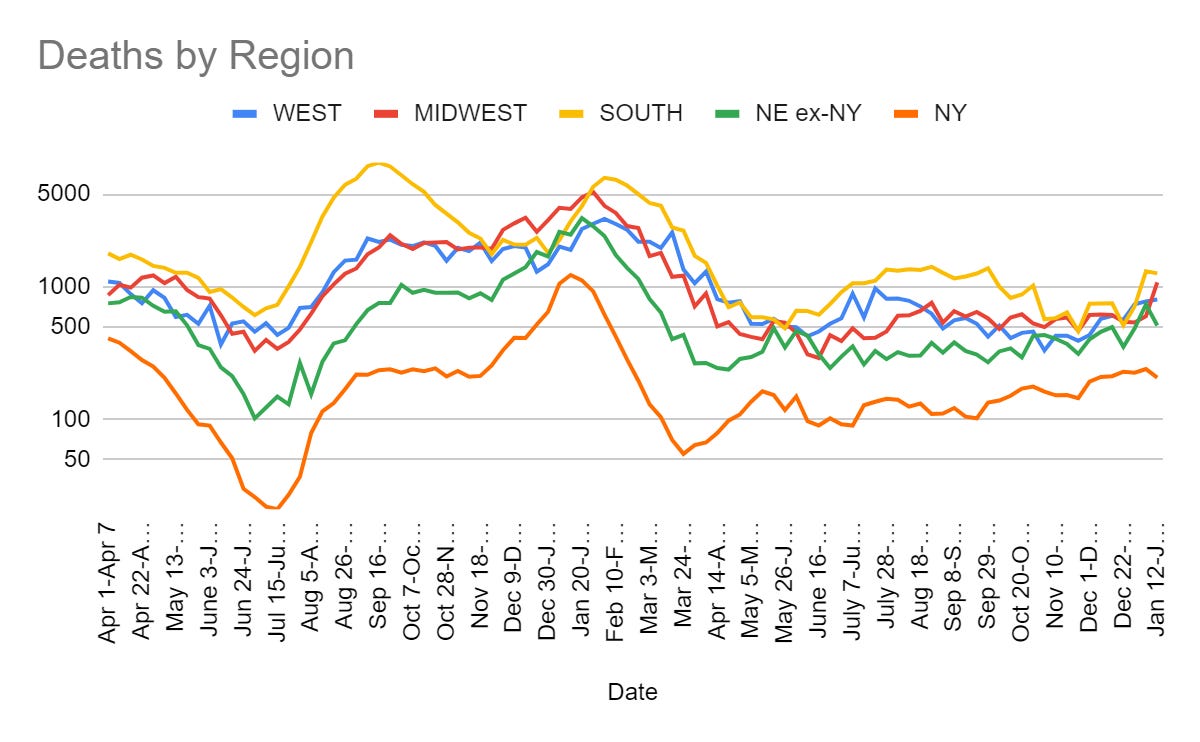
Deaths unexpectedly up for a second week, should be peaking here.
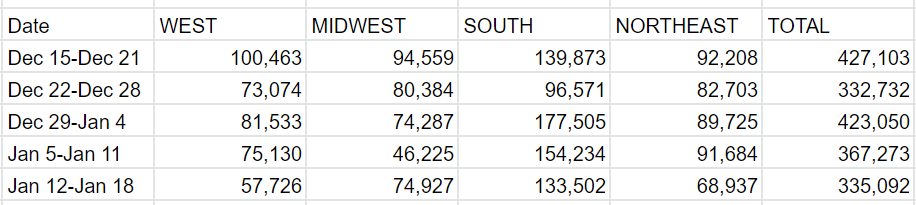
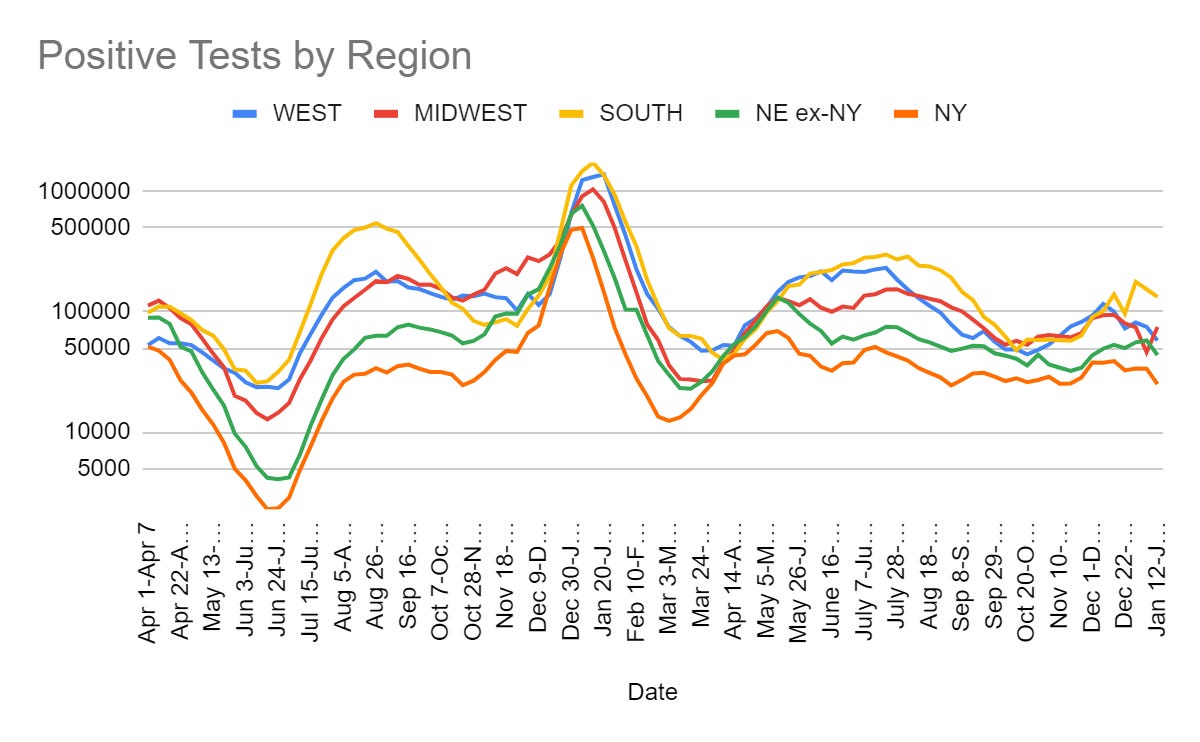
Cases unexpectedly down a lot in Northeast, other regions likely will follow soon.
Estimate says China’s wave peaked at ~3x the size of last year’s Western wave.
Let’s run the numbers.
The Numbers
Predictions
Predictions from Last Week: 385k cases (+5%) and 3,100 deaths (-15%), which I noted had high uncertainty and I didn’t even remember that there was MLK Day – when I am adjusting for a future holiday, I explicitly note that.
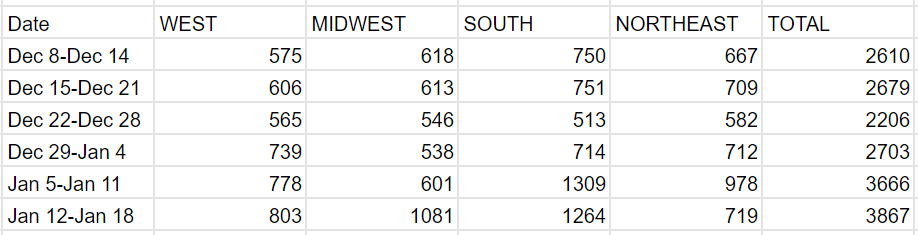
Results: 335k cases (-8%) and 3,867 deaths (+5%), the reverse result.
Predictions for Next Week: 320k cases (-5%) and 3,600 deaths (-8%).
There were a number of states reporting obviously time-shifted results in both directions. I chose not to adjust any of them other than Florida’s 2-week cycle.
Thus, the rise in the Midwest is mostly due to Illinois and Indiana reporting all of last week as part of this week, but even with a one-sided fix we still see that the higher level of deaths maintained itself despite the holiday. The increase in deaths seems real, yet so was the decline in cases. I got this one backwards. So things were recently modestly worse, but they should get better from here.
Deaths
Cases
Physical World Modeling
Celine Gounder notes that we did not have a winter surge in hospitalizations or deaths, attributes this to immunity built up over time. That is in spite of XBB.1.5. She also has a thread of the latest evidence on boosters that is more of the same. There is a modest spike in deaths the last two weeks, but nothing that implies exponential problems, especially with the Northeast already seeing large case declines.
Even more than that, in the US states dominated by Omicron XBB.1.5, hospitalizations are already plateauing.
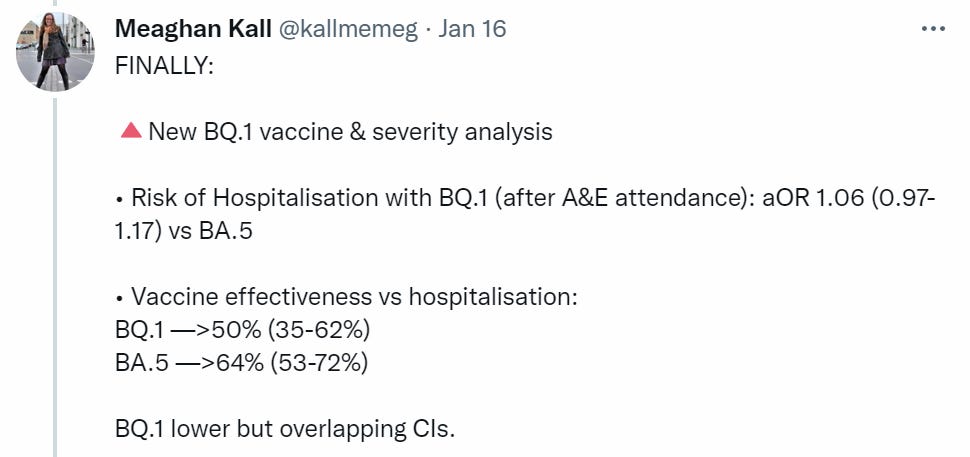
Meagan Kall goes over the latest UK technical briefing. BQ.1.5 has the replication edge over other variants, as we presumed. Here’s vaccine effectiveness, which remains substantial but may be down somewhat.
Bloom Lab speculates on future Covid-19 disease burden based partly on our experience with other viruses. Expects lower burden over time for most people due to prior infections, but perhaps not much impact for the elderly, which unfortunately is where most of the risk lies.
Zeynep Tufecki notes that in a meta-anlysis of Covid cardiac symptoms, out of 106 studies, only 6 had representative samples. The others were essentially worthless.
In Other Covid News
Ryan Bourne reports on the nonsensical policies of the AEA conference, which required masking and proof of a booster, while being held inside a hotel packed with unmasked guests, with the under-40 crowd mostly complying and the over-50 crowd mostly not complying. As a result of some mix of the masks, the selected topics (a lot of climate, race and gender papers and discussions, not so many on inflation or growth), the ability to stay home and the lack of feeling that one would suffer for not showing up, not many showed up and the conference lost a million dollars. That all sounds like quite the failure of economics.
China
Scott Sumner reminds us of the obvious fact that China did not previously have a major Covid outbreak and cover it up, as there would have been no way to cover it up. Also the obvious fact that Covid Zero was a clear and highly expensive politically-motivated error.
How big did this wave get before peaking? Here’s an estimate (preprint).

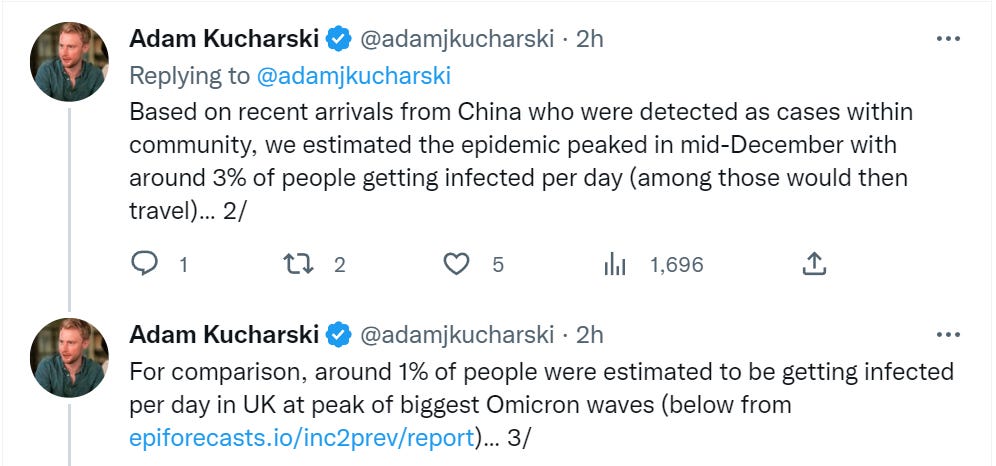
I’d also suggest that catching Covid negatively impacts chances of travelling in the short term, although by contrast being inclined to travel likely increases infection risk, and that Beijing likely got hit unusually bad the way NYC did.

Huge error bars everywhere, but peaking at several times the peaks we had last year in Europe seems plausible to me under the circumstances. Given that you can only infect 3% of the population a day for so long before you infect everyone, we should now be well past the peak in at least many areas.
Remember
Did you know mask mandates that say “you are required to wear a mask” are more like… suggestions? This is in reference to the AEA conference:
But Olney’s response was shocking.
She wrote:
Huh? I’m guessing that means you’re not here. Like all mask mandates, it’s more a suggestion than anything else. As is true everywhere. Take care of others, or do your own thing. Your choice.
To be fair to Olney, a substantial number of people disregarded the requirement and the rules were not enforced, as noted last week. That does not make this better. If you institute requirements, enforce them. If you don’t want to enforce them and they’re more like ‘suggestions’ then I suggest that, instead, you suggest them. Otherwise, you are punishing those who think your words have meaning and that your rules need to be followed, and you are sending the strong message not to follow your rules.
This also applies to everyone else, especially governments.
Other Medical and Research News
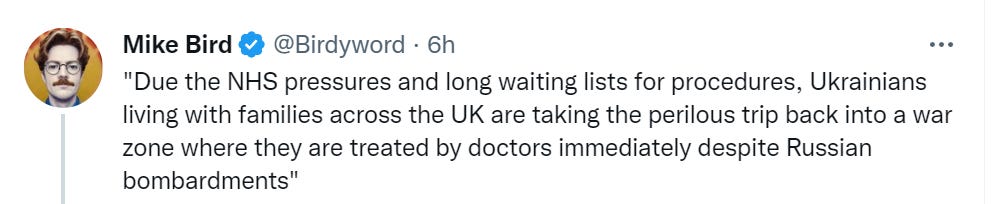
How bad things are getting for the NHS, a continuing series.
A simple and highly plausible case that iron deficiencies are very bad and you should treat them. My understanding is that magnitude matters, so not all cases are a big deal, but some cases are a very big deal and it is a cheap action to check if that means you.
Tl;dr: If you are vegan or menstruate regularly, there’s a 10-50% chance you are iron deficient. Excess iron is dangerous so you shouldn’t supplement blindly, but deficiency is easy and cheap to diagnose with a common blood test. If you are deficient, iron supplementation is also easy and cheap and could give you a half standard deviation boost on multiple cognitive metrics (plus any exercise will be more effective). Due to the many uses of iron in the body, I expect moderate improvements in many areas, although how much and where will vary by person.
This is quite a lot of prescriptions (source) for something that is almost, but not quite entirely not unlike meth.
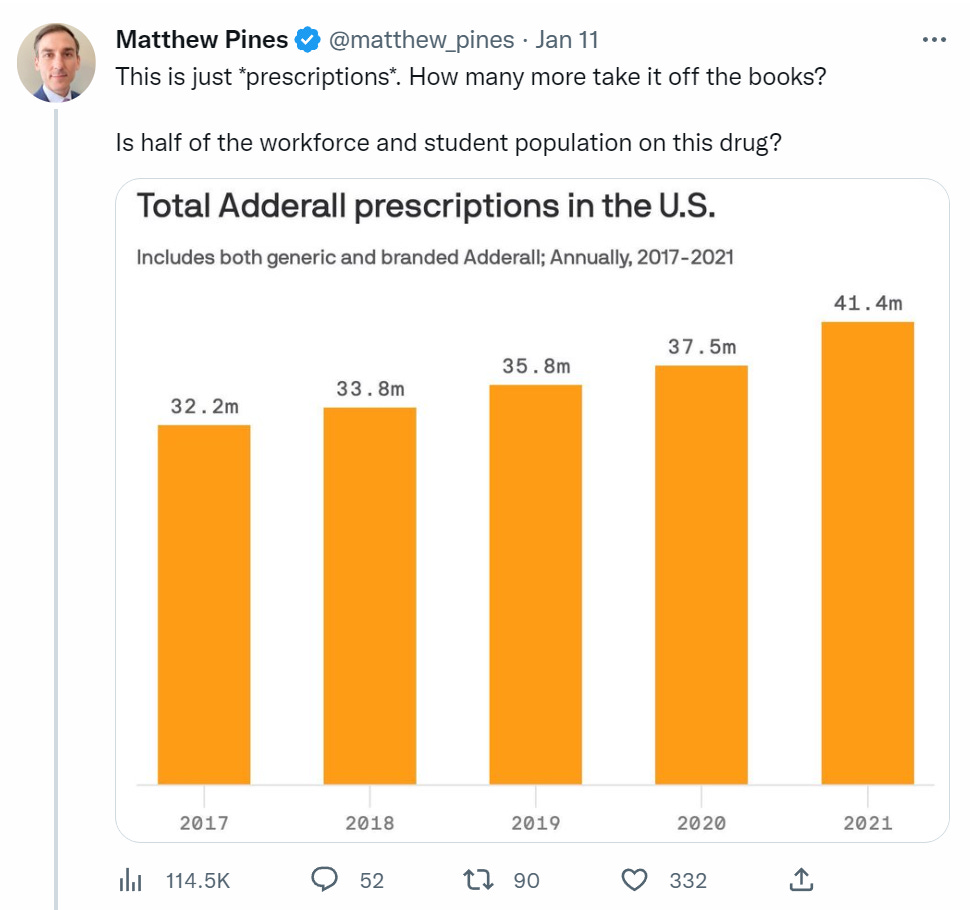
The shortage is, as I understand it, entirely induced by restrictions on supply. If you are going to give people prescriptions like this, you owe it to them to let them easily get their fix. At the same time, if we are giving out over forty million prescriptions for this, multiple things are deeply wrong.
Another visualization of the key predictor of obesity is not genetics, it is what year it is.

Forty million prescriptions doesn’t seem like a lot, given that (as I understand it) these prescriptions are not permitted to be for longer than one month supply. It would imply that around 1% of the population are on this drug (legally) at some given time.
I would be a bit surprised to find that the graph was summing over monthly prescriptions to display an “annual” total.
Separately, 1% seems deeply incongruent with my observations. I would have a much easier time believing 12%, though indeed that does seem a bit high since it includes age brackets which are very unlikely to be taking it.
Getting good numbers is a little tricky. This study claims that 16 million adults used prescription stimulants in 2016, which does technically allow for the possibility that they were on it for one month in that year and would still have been counted. It also says that “Fifty-five percent of total prescriptions in 2015 were to adults age 20 and older”, which lines up well with the 32mm figure in the graph above for 2017 (across the entire population, not just adults).
Edit: anyways, my final take is that I very much doubt the average adderall prescribee only gets it for one month per year, so I think the true number is in fact in the 40mm+ range.
The Bloom lab thread about how elderly may not improve in terms of mortality while the younger population does could be at least partially confounded.
It uses graphs from the 1918 H1N1 flu, and the 1968 pandemic invasion of H3N2 into the human population.
The work of Michael Worobey and company strongly suggests that the first flu you are exposed to, and to a lesser extend the whole ensemble of immune memory you have built up, strongly affects your response to other novel flus for the rest of your life. Specifically, they have evidence that the odd age distribution of deaths in the 1918 pandemic was because people in their 40s onwards had pre-existing immune memory to H1 flu viruses from their childhood while younger adults did not, and so to those young adults it was a high severity novel virus while to the elderly cohort it was much more like an ordinary seasonal flu.
They have weaker evidence from serum samples rather than viral genomes that between 1890 and 1900 H3 flu viruses circulated in the human population. People older than 68 thus would have at least some immune memory against the new virus, which could skew their initial mortality downwards compared to something completely novel. Note that the split used is for those under/over 65.
In short, in both of these circumstances the young population was definitely seeing a novel virus they had never seen before, but in probably one and quite possibly both of them the elderly population was already prepared by immune memory from childhood and you would expect it to be much more like ordinary seasonal flu.
The 2009 swine flu was another relevant circumstance—it was a new H1N1 flu invading the human population from pigs, with a common ancestor with the H1N1 already in humans a century in the past so the drift was more than enough to make sure that we were all very easily infected. This lead to bizarre disease dynamics for more than a year, people getting sick all out of season in multiple waves. But deaths were barely above a normal flu season, because even though the similarity was not enough for immune memory to reliably prevent infection, it held off severe disease.
Unlike all of these circumstances, no one of any age who didn’t already have SARS had any relevant immune memory to SARS-2.
The 1951 Liverpool virus described is fascinating.
ZT tweet about only 6 of 106 studies seems to link to the wrong tweet. Might want this one instead.