The majority of this week’s post is various people doing their Obligatory Thread on Latest Variant, in this case XBB. All reach broadly compatible conclusions:
XBB is the next variant and rapidly taking over, and this is normal.
XBB is not more deadly.
Our existing protections against severe disease and death carry over.
Our existing protections against infection are reduced a lot.
XBB is not obviously going to result in more infections over time.
All the standard Public Health recommendations remain in effect.
Executive Summary
XBB is taking over.
XBB is no more or less dangerous than previous variants.
It will however extend the winter wave longer than it would have lasted.
Let’s run the numbers.
The Numbers
Predictions
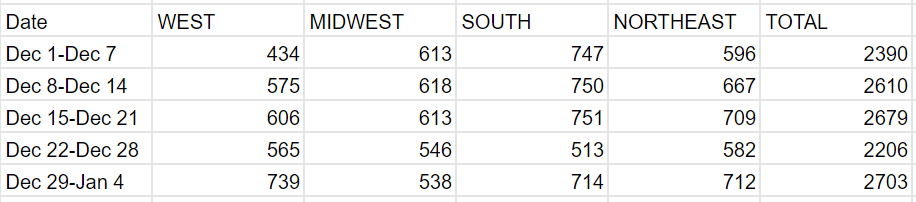
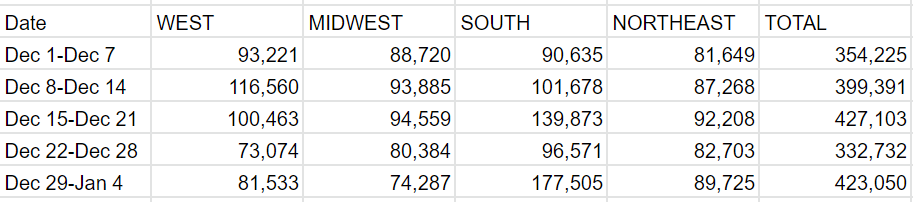
Predictions from Last Week: 385k cases (+16%) and 2,600 deaths (+17%)
Results: 423k cases (+27%) and 2,703 deaths (+23%).
Predictions for Next Week: 450k cases (+7%) and 2,950 deaths (+7%).
The numbers came in higher than expected, more due to the standard ‘data is funky so hedging my bets’ factor than anything on the ground. This next week we will smooth out the double reporting in the Carolinas and other back-fills, while making up for New Year’s, so it’s another funky week.
Florida failed to report for the second straight week. I’ve given them the same numbers I gave them last week.
For all the talk of a wave, so far we have not seen a substantial spike in deaths. This week’s numbers are not much higher than early December, instead they are reverting after Christmas.
North Carolina and South Carolina clearly reported two weeks worth of data, adding about 30,000 cases and 100 deaths that should instead be part of the previous week. I did not adjust for this as it is part of the standard holiday cycle. Thus, the case numbers in the South should not be alarming.
Deaths
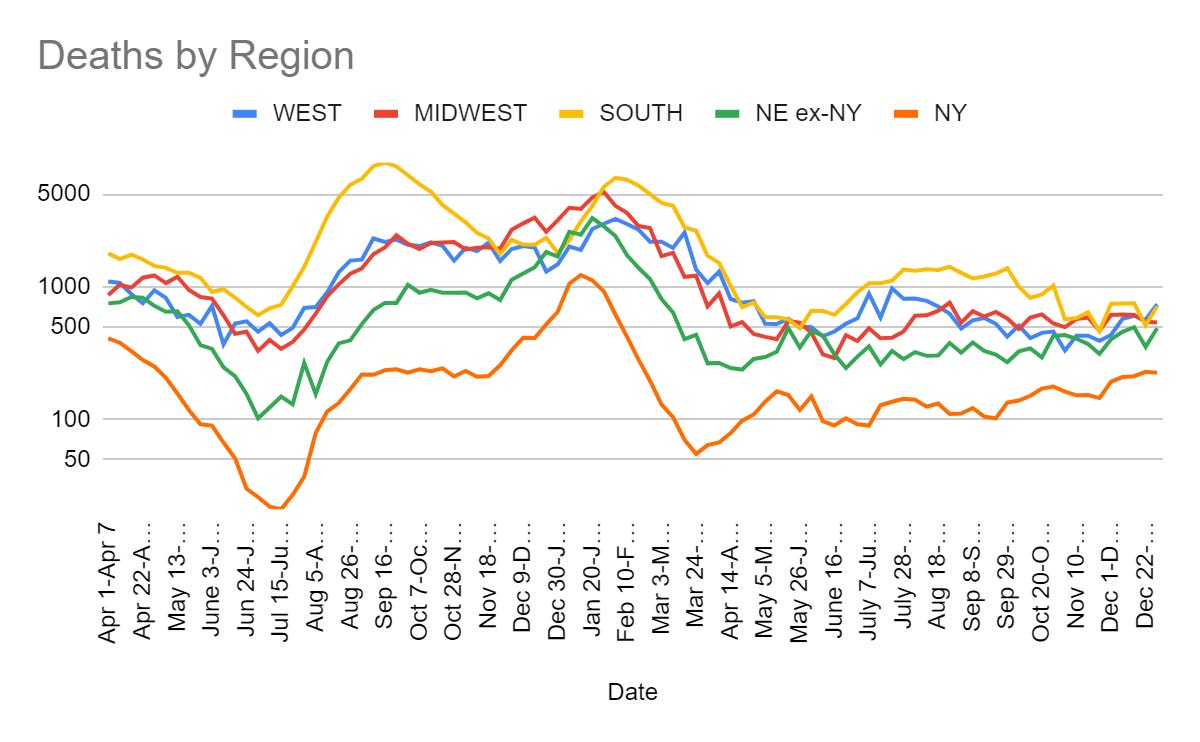
Cases

Bob Wachter notes that Covid asymptomatic positive test rate in SF declined from 5% to 3.2% on December 30. He notes that this is likely a temporary lull, partly due to XBB.1.5. It is still an excellent sign that we were at least close to stabilizing before that.
Caitlin Rivers joins the camp that says case numbers are no longer that useful, says that our case numbers have become almost completely decoupled from other indicators.


I agree that there is danger when comparing case numbers now to case numbers a year ago. I still think that comparing to last week is highly useful, as the reporting regime will have changed little. Thus, I still see them as useful, as long as they are combined with a metric that does not have this problem, such as deaths. As I’ve noted, wastewater and hospitalizations are useful while having their own problems. Test positivity depends on who gets tested and why, and which tests are reported.
BNO reports hospitalizations are their highest since February. This was well after the peak of cases last year.

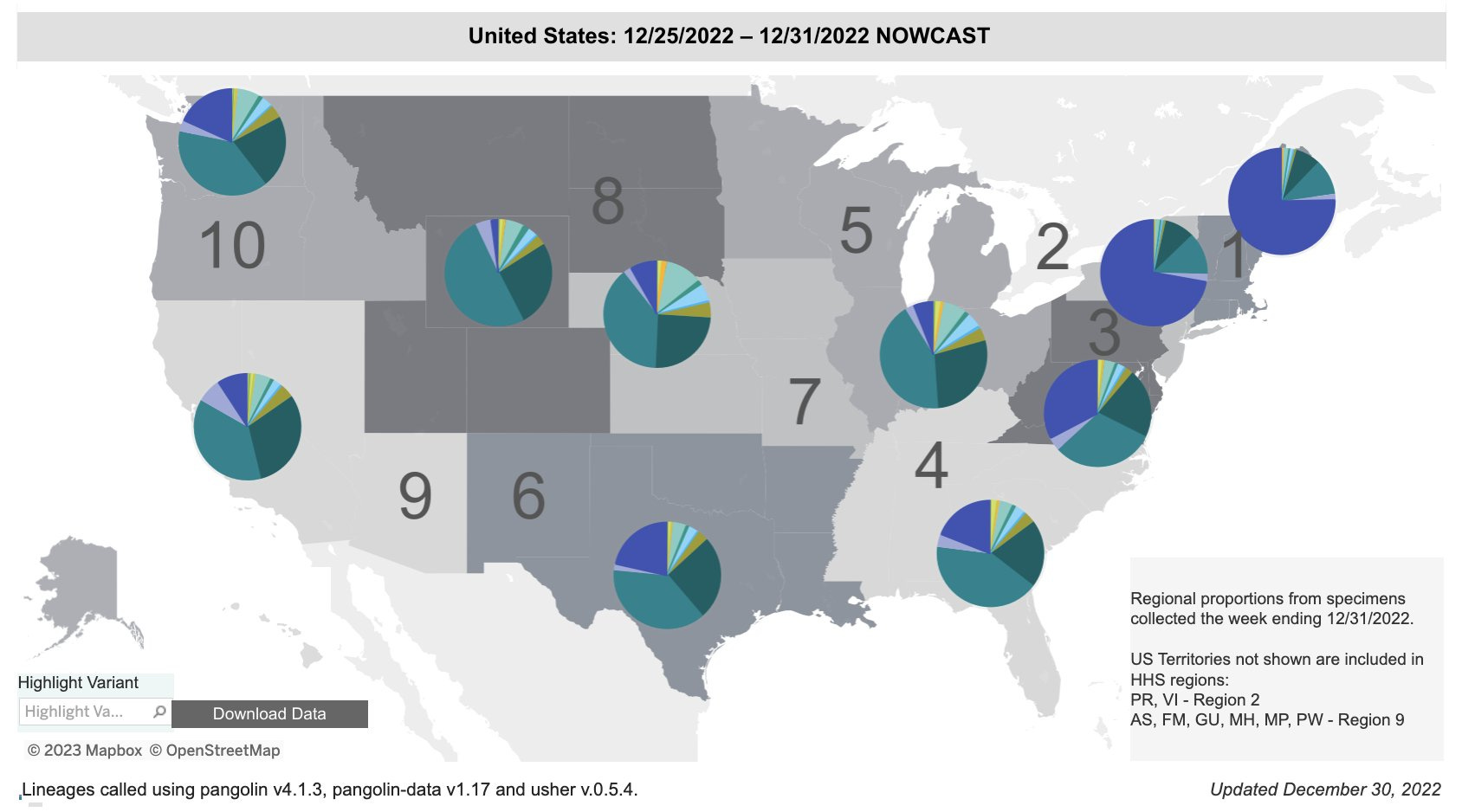
From the nowcast of about a week ago, the spread of XBB.
Here’s wastewater monitoring.
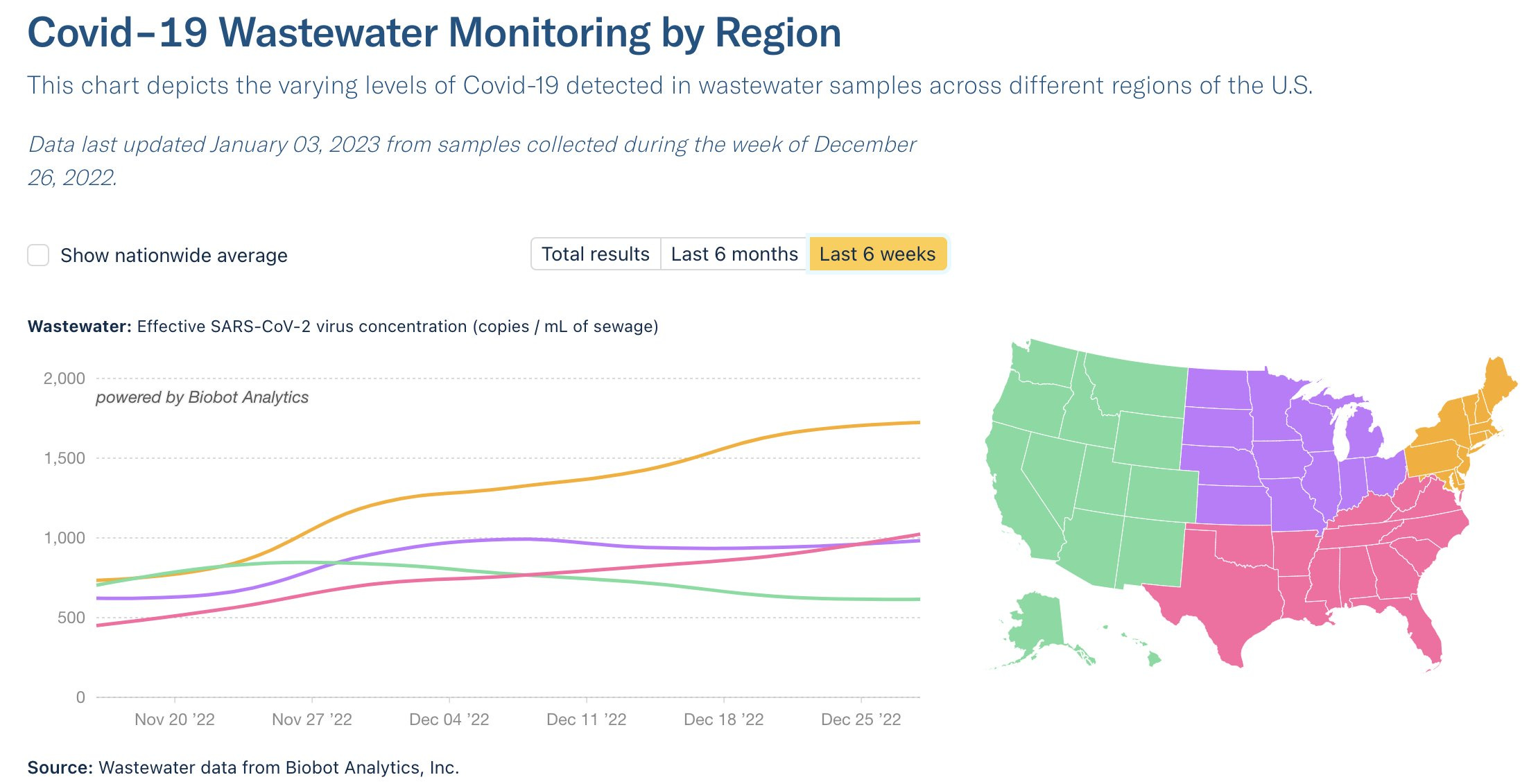
That shows the west in decline up until about a week ago, and even the Northeast only going up a factor of about 2.5.
XBB.1.5
New year and variant, who dis? (preprint)
In summary, XBB.1.5 is highly immune evasive and is spreading due to this, it is not more dangerous than previous Omicron variants, and the bivalent boosters and recent other infections (while not ideal) still prevent severe disease – if that’s all you need to know you can skip the section.



The good news is that it seems the advantage of XBB.1.5 is mostly that it is better at immune escape, and that it is if anything even less inherently dangerous than previous Omicron variants. That means that we will have a wave once again, but that our situation did not become permanently worse. Once we cycle over again, we’ll be back where we started, and with one less plausible escape candidate mutation waiting for its chance.
Eric Topol asks point blank the important question: What can be done about this?
Alas, the answer he comes back with is, essentially, nothing. The boosters are still likely better than nothing despite the immune escape. That’s about it.
Once again, in an adequate civilization this is exactly when we would rush out a new updated booster for XBB.1.5, ideally not bivalent at all, so those who were vulnerable or otherwise wanted to be protected could take it.
Needless to say we are not going to do that. We are not talking about it. I have yet to hear anyone even mention the theoretical possibility that we could respond to a new variant that had immune escape by trying to vaccinate people before they could get infected. At which point, it is reasonable to ask what we are even doing. In practice, our vaccine update plan has utterly failed and is capturing almost none of the available value.


I have no idea what policy action is being suggested.
Something must be done.
???
Therefore we must do it.
What would even be something?
The second best time to plant a tree is right now. Won’t help in an emergency.
Chise is here, same as every week, to remind us that immunity remains a thing.





This says that XBB.1.5 is spreading faster than XBB.1 due to much higher hACE2 binding ability.
Here is another relatively worried report, although the most important fact – no increase in severe disease – is again confirmed.




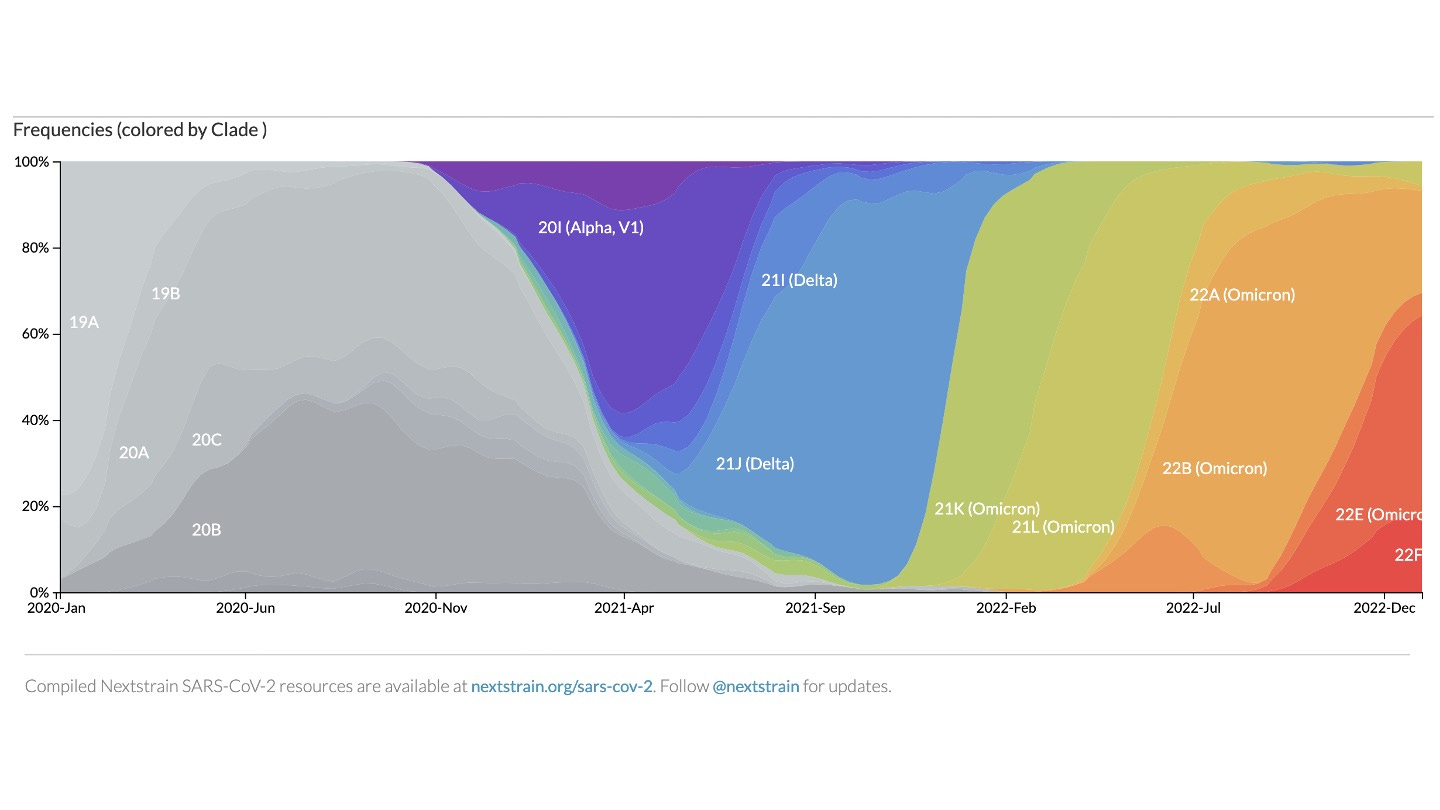
I like this visual explanation of the history of variants, via Bloom Lab. Full thread doesn’t have a strong opinion on whether new variant will increase total cases. Does include a bunch of detailed genetic information on XBB. Makes it sound like this is mostly an evolutionary trade-off that does not obviously make things generally worse.
FDA commissioner has a thread about XBB and vaccines (study mentioned).
‘No clear evidence’ is an interesting twist on No Evidence. I notice that I very much did not update the way Califf would have liked me to when I saw it, as my brain interpreted it as a Double Weasel and based on what I know I would have expected him to be comfortable saying something far stronger. Not sure why he didn’t do so.
(Also he seems clearly behind the times on the ‘will move to other regions quickly’ bit, XBB is already everywhere.)
Yes. I agree that it is highly likely the existing vaccine and booster are helpful in preventing serious illness and death.
It is also all but certain that you and the agency you head, sir, are the reason we don’t have a more effective updated booster on the way sooner. It is on you that by the time we get a booster that works it will be too late to do much good.
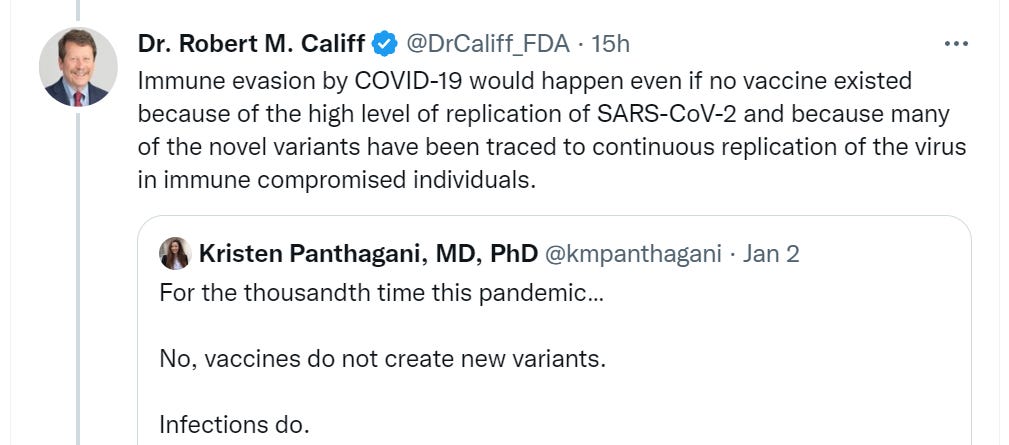
I notice this kind of talk is engineered to silence the opposition and protect against possible objections to vaccination rather than seeking understanding. Do vaccines raise or lower the probably of a new variant emerging? It can go either way, depending on vaccine impact on several things including severity and spread. Using the Authoritative Dismissal like this likely only backfires.
And now, Saying the Quiet Part Out Loud.

‘We are concerned that raising doubts about the value of vaccines will continue to lead well-intended people to delay getting an updated vaccine.’
This is not the suppression of misinformation. This is flat out saying:
People who notice certain true things don’t act how we want them to.
We recommend you don’t talk about those things, or ask questions.
We recommend you instead act how we want you to act.
I for one appreciate the honesty.
Gounder tries to thread the needle on ‘fully vaccinated.’
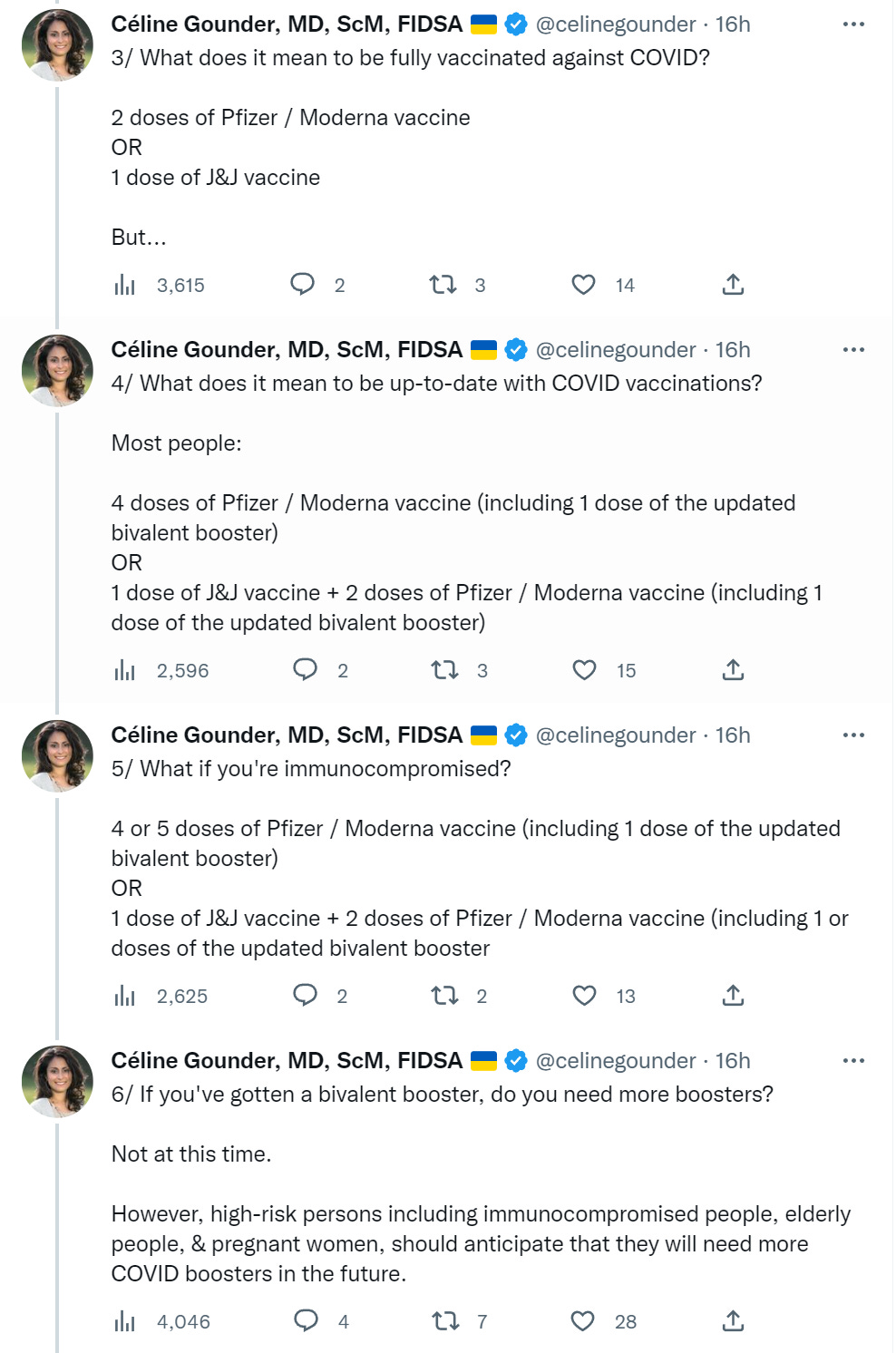
She wants it to be one way. That would be good. Instead, goalposts are being moved, and most sources have moved to ‘fully vaccinated’ meaning what she calls ‘up-to-date.’ It is interesting to see a defense of the old classification system.
Also, once again, do you need more boosters? No, you need – if you want maximum protections – an updated booster that targets XBB. Which Dr. Califf is keeping illegal.

My model continues to think that vaccination reduces Long Covid risk per infection because it is proportional to severity. I continue to be unable to take seriously anyone who takes ‘42% Long Covid risk’ seriously.


This is not how I would interpret the case numbers or wastewater graph, nor would I engage in the typical ‘you could have Done More’ routine. Yes, cases in lots of places are ‘up’ because it’s early January, but clearly the primary driver at this point is XBB.
Ashish Jha thread on XBB, essentially saying we know enough that this is unlikely to be a huge setback but still don’t know much, and suggesting the usual interventions.
Marc Veldhoen thread on XBB. There’s always a new variant, hospitalizations look proportionate, our defenses against severe disease are holding.

Physical World Modeling
Matthew Healy offers a Google Document aptly called Key Covid Metrics and How to Compare Them. It also explains a bunch of his reasoning and how he thinks about the pandemic. Kudos to him for writing this up.
The major sources of information he follows, formatted the way I do such things:
US Wastewater SARS-CoV-2 virus concentration numbers from Biobot.
US Reported Deaths and Hospitalizations, and many epidemiological forecasts, from Covid19ForecastHub.
US Excess Deaths and World Excess Deaths from OurWorldInData.
Reported hospitalizations and deaths in various parts of the US from Covid Act Now.
The truly superb blog Your Local Epidemiologist by Dr. Katelyn Jetelina.
Many deeply informative talks by one of the world’s top experts on the evolution of viruses at Bedford Talks. Note: it’s not obvious how to go from slide to slide in Dr. Bedford’s presentations! On a mobile device, drag left and right. On a laptop computer, use the left and right arrow keys.
The Twitter feeds of several dozen experts in various aspects of Virology, Epidemiology, Infectious Diseases, and related fields whose Tweets I have found to be especially valuable, with a warning that one needs to be able to discern who is worth listening to and who is not, and this is hard.
He then discusses how he thinks about these metrics.
His first metric is wastewater data. He attributes the rising ratio of wastewater data to reported cases to the rise in home tests that are not reported. I would also include that people are getting less sick and are less concerned about it, many more cases are outright asymptomatic, and many more cases are not even being tested.
I also wonder about whether different variants create different relative amounts of virus in wastewater. It seems plausible, for example, based on the details we know, that a given Omicron case could generate a larger wastewater signature than a pre-Omicron case. I’ve seen no attempts to measure this and find out. I haven’t talked about that concern. I’ve had it for a while. It’s been one reason I haven’t relied as much on wastewater measures.
Another reason is that I have a system I have learned to understand and navigate, which I then supplement with wastewater data, and found it easier to allow path dependence here. I was confident (and still am) that if there is a big divergence between measures I will notice and think about it.
He also looks at hospitalizations. I used to do that a lot, then I got frustrated by the degree to which capacity constraints and policy decisions were warping that data, and concluded it had stopped being useful.
Whereas he does his best to avoid case count data, I presume due to the lack of reporting and data integrity issues. If I was starting from scratch without my experience navigating those numbers, I might do that as well at this point.
He estimates 50% of America will be infected by Omicron in its first year or so.
He mostly thinks excess deaths are a better measure than reported Covid deaths, since almost all deaths are reported while cause of death is not as reliable, and takes it as relatively safe to say that excess deaths equal Covid deaths.
One note he makes is that most excess deaths post-vaccine were in red states, and he estimates that Trump ‘embracing scientific reality and strongly urging people to get vaccinated’ could have saved 400k lives. I don’t think it was within Trump’s power to close the majority of this gap, because I don’t think people would have listened even to him, unless other big changes are also made, such as him remaining in office, or everyone working together and releasing the vaccine pre-election, or complete sea changes in messaging and distribution from public health. Otherwise, a majority of what happened was effectively baked in.
He then highlights some papers.
He cites this paper as important, emphasizing the roll of county-level political affiliation and its correlation to excess deaths, and that state governments that enforced their restrictions narrowed these gaps.
He cites this paper that says that developing countries had double the death rate from Covid when adjusted for population age, the pre-vaccination infection fatality rates (IFR, not CFR) between developed and developing countries were similar at 0.5%. I would also consider quality of data and case reporting here.
Finally, he cites this study of individual level data in Ohio and Florida, showing excess death rates for Republicans were 76% higher than those for Democrats, widening from 22% pre-vaccine to 153% post-vaccine, concentrated in counties with low vaccination rates, so most of this effect was presumably due to vaccinations. This is a big argument for the value of vaccination, while also being somewhat of an argument against the importance of NPIs.
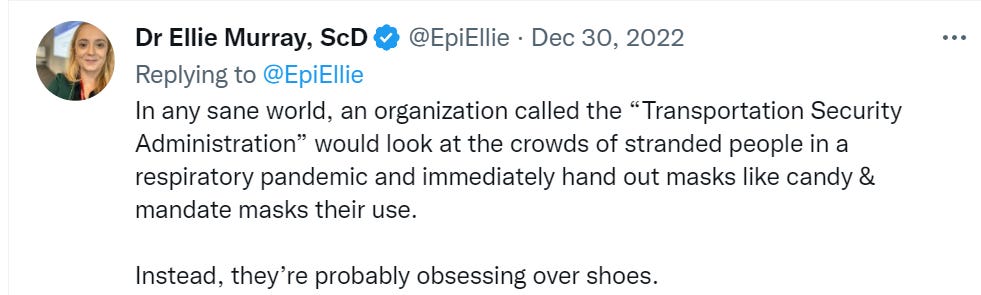
An excellent contrast. I wouldn’t be mandating masks anywhere at this point, but if I did terminals would be near the top of the list. I’d certainly be handing out KN95s all over in such places to whoever wants them, it would doubtless net save money. If you want to make air travel safer, focus on the terminals.
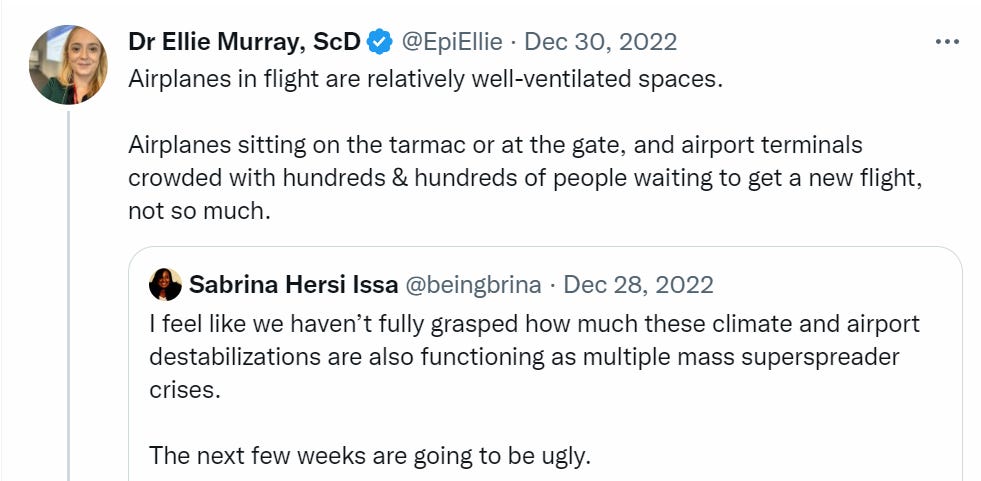
I should also note that I don’t think Issa is right about the magnitude of these effects. It’s easy to focus on conspicuous failures and hot spots that involve relatively few people, rather than focusing on the everyday interactions and other dynamics that matter far more. The next few weeks are likely to be somewhat ugly, but that would mostly be due to timing and XBB, and only a tiny bit about airports. There simply aren’t enough travelers involved to matter that much here.
Analysis of latest study on surgical versus N95 masks, finds non-inferiority for surgical masks, which in practice performed only slightly worse well within margin of error. There are still lots of reasons to presume N95s are the superior technology if all you care about is prevention, but this closes my estimate of the effectiveness gap, and the degree of discomfort matters. A doctor who feels, as one is quoted as saying, that their ‘head is in a vice’ by the end of the day is not going to be on top of their game.
Booster Boosting
The good news is that even the University of California is now willing to let you opt out of Covid vaccination. The bad news is that to do so you have to attest to being ‘aware of the following facts.’

The good news still vastly outweighs the bad news. If you are going to the University of California, you are doubtless used to and accepting of being forced to consistently attest to things that you do not believe.
Permanent Midnight

The comments include quite a lot of very explicit support for Permanent Midnight. Remember. Also remember to give thanks that Public Health types did not win.
They continue their quest to make all other voices illegitimate.
In Other Covid News
China
Not Covid, seems worth including anyway.
Morocco outright bans travelers from China due to Covid risk. This won’t meaningfully help Morocco avoid Covid. Still, China did kind of ban travelers to China for several years, so… fair.
I continue to not understand what people mean when they say, as in this video clip from MSNBC, that call for ‘collaboration’ or claim that ‘Xi needs to slow things down’ or otherwise that there is anything China could still do. It’s over. It’s done. Whatever is going to happen essentially can no longer be changed.
Remember
Bryan Caplan looks back on the libertarian reaction to Covid. I agree with his framing of there being essentially two camps, those who advocated for freedom to protect ourselves from Covid (he calls this ‘tech freedom’) in ways that make sense, and those that advocated for freedom against Covid protections (he calls this ‘personal freedom’ although that doesn’t seem like a clarifying term to me) that didn’t make sense. As he notes, these are fully compatible positions – freedom to do what you want and freedom to not do what you don’t want.
Yet most people only advocated mostly one or the other, and the two camps got into arguments. Caplan says that both camps ‘lodged some fair complaints against the other.’ The complaints by the tech freedom side were largely about vaccine skepticism. He doesn’t mention these, but I’d throw in complaints about their frequently advocacy for things like Ivermectin, unjustified skepticism of the effectiveness of NPIs, and often portraying the ‘focused protection’ or non-intervention scenarios as far less deadly than they would likely have been.
I certainly broadly agree that our use of NPIs stayed far too intense for far too long, and that the expectation this will happen again is the strongest argument against allowing NPIs (or any other such ‘temporary’ intervention) to take hold in the future. Yet I think there was a serious intellectual integrity problem here.
Whereas the complaint against the tech faction seems to be that they… were complaining about vaccine skepticism or a failure to support the crusade against NPIs sufficiently strongly? I’d agree that this was often an issue, and for my own part I did not come around quickly enough when the time came, but it’s a very different style of complaint.
Ultimately Bryan cites the freedom-from-interventions cause as more important going forward, because we were exceedingly lucky to get vaccines so fast this time, and without them we risk sliding into years of tyranny. In this model, keeping life worth living is the higher priority.
There are several counterfactuals and potential future scenarios here where we likely disagree on how things work.
I expect to usually have a vaccine available very quickly in these situations if we actually care about creating it. I don’t think we got as lucky in this particular way as Bryan thinks especially now that we have mRNA vaccines, and the alternative scenario where we get vaccinated starting in May or June of 2020 is worth keeping in mind, and I think the FDA is likely to also shut out many other vital tools that would clearly return us to a more normal state faster.
I also don’t expect a Permanent Midnight scenario to take hold so easily. There is a reason China eventually gave up. The cost of maintaining these kinds of restrictions rises with time, and anyone calling for them to be sustained will get voted out, and I expect people patience to if anything be lower next time. To get such a scenario, we’d need a virus that was much deadlier, especially to younger people, that also was in the strange ground where interventions were neither successful nor hopeless.
In that scenario, I’d still be much more interested in pushing for faster vaccine and treatment development, and better tests and NPIs, than I’d be interested in fighting harder against the NPIs so we could more or less ‘accept the deaths’ and move on. The space where the opposite holds might exist, but it seems quite small to me.
Tyler Cowen looks back and finds rapid Covid tests not so important. Certainly they were not in the same league as vaccinations. I think Tyler is selling the tests short here, largely from failing to think on the right margins.
In many cases, tests enabled gatherings and events that would otherwise have not happened, because people would have not been willing to take part. This likely includes a large number of schools, as well as things like family gatherings. It allowed many high value offices to reopen. This change seems super valuable.
The idea that ‘reassuring Nervous Nellies’ is a low value use is something I’d disagree with. Making the Nellies less Nervous is highly valuable, although it must be weighed against the cost and annoyances of needlessly imposed tests on others.
In other cases, a rapid test substituted for a PCR test that would have cost the system hundreds of dollars and often required great inconvenience, while the rapid test in practice was more useful.
Even if you ‘already pretty much knew’ you had Covid, for many reasons you often needed to confirm this, and the cost of having doubts by yourself or others remained high. The gain here is not so minimal.
The bottom line here is that, in practice given our approach to Covid, availability of cheap and quick rapid tests was a very large welfare improvement in lived experience and productivity. I am confident our children would have been in school far less often without such tests.
What about the prospects for mass testing or periodic testing? That depends on solving for the equilibrium, and what other things then happen that balance out the decrease in risk from the tests, and how much lower overall infection levels are before they stabilize, since full suppression was never viable. I do think we missed opportunity here.
Thus, I continue to think the value of rapid tests, and the value lost through our failures on that front, was quite high.
Other Medical and Research News
A study from 2015 on how often families with small children get respiratory infections.
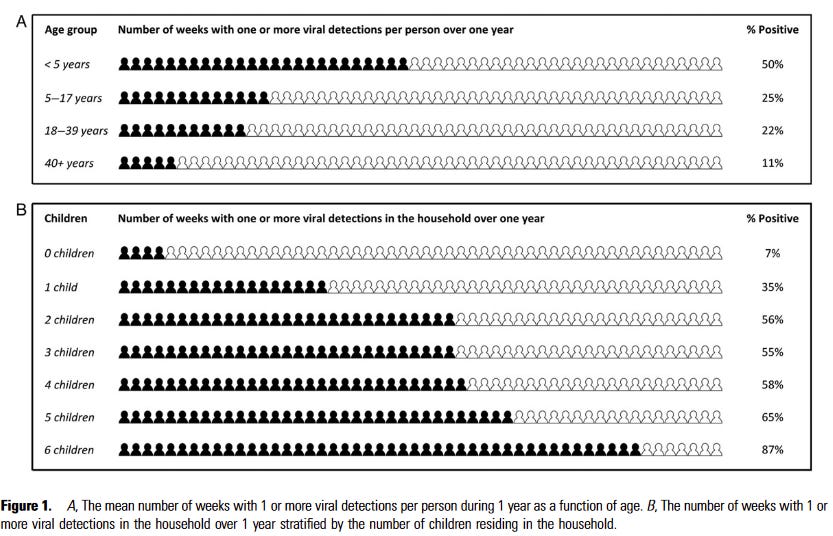
The correlation here between children is very high. Either there is a bug ‘going around’ or there is not. Once you have two children, the chance one of them will get whatever is going around is already very high, so adding several additional children does not change things much, except insofar as they then infect each other, but even that effect seems likely to be small here.
Reminder: Claims that ‘the number one cause of obesity is genetic’ (study) and there is nothing anyone could do to prevent ‘this disease’ do not pass the laugh or smell tests. This is Obvious Nonsense .
On top of the data, there is the simple fact that not too long ago few people were fat. If the primary cause of being overweight was genetic, we would not suddenly go from mostly not fat people to quite a lot of fat people. That is not to blame anyone, simply to say that whatever is happening, this isn’t it.
GDPR so restrictive it is driving research out of Europe (FT).
If you have to deal with Europeans, Because Internet, it is hard for outsiders to understand how huge a pain in the ass and drag on productivity it is to have to follow GDPR. Perhaps something where you have a choice, like clinical trials, will reveal the depths of this damage.
Canadian Assisted Suicide
Richard Hanania makes the case for Canada’s assisted suicide program as moral progress, and, well… I appreciate the frankness.
It is true, for example, that some people might feel “pressured” to commit suicide because they don’t want to be burdens on their families or the government. I don’t think there’s anything wrong with this — in practically every other kind of situation, it is usually considered pro-social to care about the impact your life has on others.
Oh, sure. Seems fine to have society pressuring people to kill themselves because they are a burden to others. As long as it’s voluntary. Here he says ‘feel “pressured”’ yet the argument logically extends to actual exertions of pressure including by officials. Which are very much A Thing.
Relatedly, I argue against the “culture of life” argument on the grounds that we place too much value on human life and it would be better if we placed less on it, a view that conservatives implicitly hold on topics like covid restrictions.
All right then.
Given the amount of misinformation that is out there on the topic, it’s important to start with some numbers. According to the Canadian government, there were 10,064 MAID cases in 2021, which represented 3.3% of all deaths in the country.
He says this is not a lot. To me it sounds like a lot.
Canada recently expanded its assisted suicide program to cover those without a terminal condition, a fact that has gotten a lot of attention, but in 2021 only 2% of deaths fell under this new category.
So out of every 10,000 people that die in Canada, 6.6 killed themselves through MAID without a terminal condition. Again, that sounds like rather a lot.
About 81% of MAID recipients had received palliative care, and 88% were eligible for it.
I read this as ‘12% of MAID recipients were eligible to kill themselves but not to get palliative care’ and also I presume a lot of the 7% that were eligible but didn’t get it had issues with practical access and waiting lists. Of every 10,000 deaths in Canada, this is saying that 37 killed themselves through MAID while ineligible for palliative care. So there is an 0.3% chance this will happen to YOU.
Once again, this sounds pretty terrible?
Richard’s core argument boils down to Yay Individual Liberty, and that there are a lot of people out there suffering quite a lot. These are important points. My main takeaway, however, was that yes the whole thing already, in its current state, seems rather terrifying.
You use the phrase “Permanent Midnight” a lot, but it seems highly ambiguous between (1) mandatory masks all the time for everyone, (2) some individuals choosing to wear masks all the time, and (3) social norms that endorse mask-wearing in some but not all situations (when one has a respiratory illness; when in a crowded ill-ventilated place at a time when there’s a lot of respiratory disease around).
Of these, #1 seems obviously very bad; #2 seems obviously perfectly OK; #3 seems like it could be good or bad or both depending on the details.
A concrete example: there’s a link to a Twitter thread starting with a tweet from Denise Dewald. In that thread I see lots of people saying things that amount to “I wear a mask all the time and I think people who don’t are being foolish”. I also see quite a lot of people saying things like “Masks do nothing at all” and “Masks lead to low blood pH which gives you cancer”. Quite a few saying “I never wear a mask and I never get sick”, quite a few saying “I have been wearing a mask all the time since the start of the Plague, and I’m getting way fewer other respiratory infections”, etc., etc., etc. I didn’t see one person calling for any mandates requiring mask-wearing. I did not read all the tweets (life is too short) so I might have missed some, but there’s certainly not much of that in the thread.
Maybe some of those people privately believe that there should be such mandates. But if any of them are saying it out loud, I didn’t spot any of them in maybe 10 minutes of trawling through a very boring Twitter thread, and the craziest mask-related opinions in the thread were anti-mask ones not pro-mask ones. And what you said was: “very explicit support for Permanent Midnight”. So what does “Permanent Midnight” actually mean?
He’s just saying that it’s unsustainable to have sacred values when there are tradeoffs to everything. That’s a point you’d accept for many contexts, so reacting with sneer here seems a bit unfair.
That said, I think his point would’ve sounded a lot better if he added a sentence like “placing less value on human life means we get to place more value on other things that also matter.”
The way he said it, it indeed sounds a bit dystopian – but what’s the alternative? It’s difficult to estimate what numbers for assisted suicide are “high” or “low” in the sense that matters morally. Some % of the people would’ve committed suicide also without assistance, and you’d probably agree that those people are unambiguously better off with the assistance. Then, some people would take assistance but wouldn’t want to kill themselves in the messy way. That seems very reasonable – it’s super scary and probably more traumatizing for anyone you leave behind to do it with household methods. Not to mention that there’s a risk that it doesn’t quite succeed and you’re left way worse than before! So, you can’t just go from “Some people kill themselves with assistance who otherwise wouldn’t” to “Therefore, it’s preposterous that this doctor describes assisted suicide as moral progress.”
Sometimes people want to do something difficult that they think is good for them, but they don’t dare to do it because it’s really aversive. Consider how many people didn’t ask out someone they had a crush on because they were too scared – asking out your crush is probably a hundred times easier than jumping off a bridge or hanging yourself or what not.
Unless there’s something particularly bad about how the medically assisted suicide program is implemented, I indeed consider this sort of thing moral progress.
“If the primary cause of being overweight was genetic, we would not suddenly go from mostly not fat people to quite a lot of fat people.”
This isn’t necessarily true. It could be that in environmental condition A, almost nobody is overweight, but in environmental condition B, people with a certain common genetic variant become overweight, while those without that genetic variant do not become overweight. If you measure genetic influence in condition B, you will find a big genetic influence. This is not a contradiction with lots of people suddenly becoming overweight when the environment changes from condition A to condition B. It also doesn’t mean that “there is nothing anyone could do to prevent” it—you just need to revert to condition A.
This is not a counterfactual. This is what Trump actually did! He himself is vaccinated, and he encouraged vaccination publicly, including continuing to do so after he lost the presidency. The only real complaint to make here is that he maybe didn’t do it enough, because he has the political sense not to continually advocate for something that his supporters hate. So your statement that it wouldn’t have moved the needle is obviously correct, not because we need to reason about what would have happened but because we can observe what actually did happen.
I do agree that the one counterfactual that would have mattered would have been releasing the vaccine in September or October and allowing Trump to take credit for it. But Public Health decided that opposing Trump was more important than getting the vaccine out a few months early.
I don’t understand the last paragraph. Who, exactly, could have released “the vaccine” in September or October but didn’t? At the time of the 2020 US elections, the vaccines from Pfizer and Moderna and AstraZeneca were all still in their Phase III trials. (Actually, I’m not sure all of them had even started their Phase III trials.)
Are you saying that the companies developing the vaccines were leaned on by antitrumpistas and pressured to schedule their trials later to make sure nothing got released before the US elections? If so, I’d like to see some evidence. (The more obvious explanation would seem to be that they did things as quickly as internal and external bureaucracy permitted, which did after all end up being quite a lot quicker than usual.)
Or are you saying that the best explanation for their choosing not to seek an EUA for their vaccines before even beginning Phase III trials is some kind of pressure not to do anything that might make Trump look good? Again, if so, I’d like to see some evidence. (The more obvious explanation would seem to be that they didn’t want to release a vaccine that either was harmful or was suspected to be.)
Or what?
https://nypost.com/2022/09/12/it-seems-clear-dems-pressured-the-fda-to-delay-the-covid-vaccine-to-hurt-trump/
https://www.theatlantic.com/health/archive/2022/01/fda-covid-vaccine-slow-rollout-trump/621284/
There exist screenshots of a government official actually bragging on Twitter about having delayed the vaccine in order to avoid giving Trump the credit. I seem to recall Zvi posting these screenshots at some point, though it might have been someone else. In any case, you can find many, many articles dating from late 2020 and early 2021 conveying dueling narratives about whether the vaccine was in danger of being “rushed” (Dem talking point) or whether the FDA sandbagged the process for political reasons (Trump talking point). In any case, the basic facts seem undisputed:
The vaccine approval process could have been further expedited, and if it had proceeded at maximum speed it would have been completed in September or October 2020.
The Trump administration did in fact pressure the FDA to approve the vaccine in October.
The FDA did not approve the vaccine until after the election.
Which is an interesting thing to observe, because the narrative has since switched and “the vaccine was a rush job and is dangerous” is now a right-wing talking point while “the vaccine is perfectly safe” is now the mainstream position.
Edit to add: On close read I realize that I was conflating the successful end of the clinical trials and their public announcement with actual shots-in-arms readiness. Shots-in-arms readiness would probably not have been accomplished in October in any case, given the production pipeline and distribution problems, but the announcement of the successful trials, according to multiple sources, could plausibly have been as early as September.
Thanks.
I would be interested to see those screenshots. Without some similar smoking-gun moustache-twirling, it’s not clear how to distinguish “regulators were cautious as a pretext for not giving Trump a win” from “regulators were cautious because that’s what regulators do, and this was a thing being rolled out to millions of people”.
E.g., the Atlantic article observes that using EUAs for vaccines at all was previously unheard-of because the numbers of people potentially affected are so large. The 60-day period that was used doesn’t seem absurdly overcautious to me, though I am not in any way an expert on vaccine side effects. Nothing in those two articles looks to me like good evidence for nefarious intent behind whatever level of caution the FDA adopted.
Of course it’s possible that some regulators were cautious for “good” reasons (wanting to make sure the vaccines were safe, wanting to make it harder for people to think they weren’t) and some for “bad” reasons (not wanting Trump to get electoral gains from the vaccines). It’s possible that some were cautious for both sorts of reason. It’s also (I think obviously) possible that the Trump administration’s motives were similarly-but-oppositely mixed.
Knowing what we know now about (1) the actual safety and effectiveness of the vaccines and (2) the extent to which people avoided them because of safety concerns, it’s not clear to me whether getting them out sooner would have been good or bad overall. More to the point, at the time it wasn’t known how safe and effective they would turn out to be, and it seems plausible to me that (a) cutting the wait-and-look-for-side-effects period would in fact have led to a better outcome but that (b) it wasn’t a good idea in expectation at the time, since there might have turned out to be worse side effects than there actually were.
Found it (scroll down to “Eric Topol is the worst”).
Related news article that goes over the key points
I had misremembered a few details, namely that Topol is an influential physician, not a government official. The gist remains.
There exists a less-malign interpretation here, which is that Topol might have had sincere concerns about the safety of the Pfizer vaccine. But I am not inclined to extend much charity. Topol explicitly states, repeatedly, that his goal was to “disrupt Trump’s plan” and prevent Trump from “getting a vaccine approved” before Nov 3. (Read Topol’s tweets quoted in the article, and click through to see the surrounding threads for more evidence.)
Who knows how decisive his influence was. Overall, I agree with your point that slowness is the default setting for the FDA, and that most people in the agency were slowing things down out of bureaucratic habit rather than explicit political motives, but there definitiely exist malign political actors like Topol.
So when you said
the only discrepancies between that and reality were that (1) he is not a government official, (2) he was not in a position to delay the vaccine (though it’s possible he influenced people who were), and (3) he doesn’t say anything about doing it in order to avoid giving Trump the credit.
My reading of Topol’s tweet is not “I tried to make sure Trump didn’t gain votes by making vaccines happen faster” but “I tried not to let the Trump administration exert pressure to make vaccines faster in order to gain votes”. (Those two things are fairly similar. The first difference between them is in what they regard as the default if no one exerts any pressure. The first: if no pressure, vaccines roll out quickly; pressure is exerted to get them rolled out slowly. The second: if no pressure, vaccines roll out slowly; pressure is exerted to get them rolled out quickly. The second difference between them is in who is alleged to be acting from political motive.)
Topol’s tweets (and other things) quoted in the article are all, on the surface at least, making the argument that rushing the vaccines out would do net harm, most importantly by reducing confidence in their safety. Since in fact a lot of people didn’t get vaccinated on safety grounds (even with the release timetable that actually happened) it’s hard for me to see that as very unreasonable.
Of course it’s possible that Topol’s words are dishonest, that his real motivation was all political, that the same goes for e.g. the other medical people who signed his open letter to Pfizer, and that all of them were happy to let thousands die if it harmed Donald Trump electorally. Politics is a hell of a drug. But since there’s a pretty plausible less-malevolent explanation—they really thought that waiting a bit would reduce real and perceived side-effect risk, and they thought that there was political pressure to rush things that needed countering—and since we are agreed that slowness is the FDA’s default setting, I’d want to see some evidence of political motivation and so far I haven’t.
You are right about (1), (2) strikes me as an irrelevant distinction once we’ve granted (1), and I flat disagree about (3).
Where he describes his motivation, he explicitly describes the need to frustrate Trump’s plans. He does this repeatedly. He focuses on this much more than he focuses on safety. The overwhelmingly likely interpretation, IMO, is that safety was a pretext and opposing Trump was the goal, and this interpretation is favored by Topol himself when he describes his actions as “opposing Trump” more often than “protecting Americans”.
He says he’s glad he frustrated Trump’s plans. It looks to me as if by “Trump’s plans” he means “Trump’s plans to push vaccines out before they have been adequately tested, in order to win votes”, and as if (at least as far as his explicit utterances go) he wants to frustrate those plans because he thinks pushing vaccines out before they have been adequately tested is dangerous and/or confidence-harming.
I should maybe say explicitly: I am making no claim about whether in fact Trump, or his administration, had any such plans, nor exactly what their motivations were if they did. I am just looking at what Topol’s stated motivations were, and they do not look to me the way you say they look to you. I agree that it is possible that his real motivations were more political than his stated motivations (many people’s often are), but since IIUC you are saying that Topol bragged about doing what he did in order to avoid giving Trump the credit I think it matters what his stated motivations were. And not once do I see him saying anything that’s more like “we should do this because otherwise Trump might win the election” than like “we should do this because otherwise we will be deploying the vaccines before they are known to be safe, and before the public will trust that they are known to be safe”.
Here are all the things in that MIT Technology Review article that tell us (by quoting or otherwise; unless I’ve goofed, things with quotation marks around them are alleged to be Topol’s actual words) what Topol said.
(article text) Topol [...] aimed to prevent Trump from greenlighting a vaccine before scientists could prove it to be safe and effective. To Topol, developing an effective vaccine against covid-19 is “the biggest event in our generation” and one that should be evaluated on the basis of scientific data, not political implications.
Article explicitly claims Topol’s concern is that political pressure is leading to bad medical decisions.
To prevent such a scenario, Topol led online calls for FDA commissioner Steve Hahn to resign after his agency was criticized for cowing to political pressure—and then phoned Hahn a number of times to urge him to resist Trump’s influence. Topol also targeted Pfizer, the only pharmaceutical company likely to seek approval of its vaccine before Election Day, which eventually set up a meeting for him with its vaccine team.
Hahn: Article explicitly claims Topol was complaining about political influence and urging that it be resisted.
Pfizer: No specific claims about Topol’s (real or claimed) motivation.
(Topol tweet) “We were on a path for a vaccine emergency authorization (EUA) before November 3rd. Thanks to the FDA, Trump’s plan was disrupted. That won’t happen. First real sign of the independence of FDA since the pandemic started. And that’s important.”
Not very explicit either way, but does claim that being slower about it means the FDA is being more independent which seems like a clear claim that if they’d done it quicker it would have been because of political pressure.
(article text) What alarmed Topol and other critics is that Hahn played along and badly misrepresented the facts, saying plasma transfusions would save 35 out of 100 covid-19 patients. [...] “That was the moment I decided, it’s time to become an activist,” says Topol. “I got very upset. I said he should resign or tell the truth. There was just this complete subservience to Trump.”
Topol is explicitly claiming that Hahn (FDA Commissioner) was making false medical claims because of political pressure.
(article text; referring to the stuff about plasma transfusions) “That event was fundamental,” says Topol. “I think [the FDA was] sensitive to external pressure that this cannot be tolerated with a vaccine.”
Doesn’t say anything about Topol’s stated or real motivations.
(article text) Topol says he and Hahn had several private phone conversations in the weeks following the debacle. What they said is confidential, but all signs indicate that Topol urged Hahn to defy the White House effort to deliver a vaccine by Election Day. “I came to respect him,” says Topol. “I was convinced he’d do the right thing.”
Doesn’t say much about Topol’s stated or real motivations, other than that he claimed to want Hahn to do the right thing. (Which of course is equally consistent with “the right thing, namely to keep the vaccines safe and confidence high by not putting them out prematurely” and with “the right thing, namely to avoid giving Trump a political win that might help him win the election”.)
(Topol tweet) “So the choke point here is that a company has to apply for an EUA. @realDonaldTrump @SecAzar cannot get a vaccine approved unless that happens. So our attention turns to Pfizer since it has been outspoken about its intent and timetable. 7/”
Nothing about motivation here at all. It’s part of a Twitter thread in which Topol says he’s explaining why he and some other doctors wrote to Pfizer. Later in the thread he says he believes Pfizer’s safety people “would share the concerns in our letter and want as strong an evidence base as possible, without holding up the vaccine approval, to support any vaccine’s safety & efficacy. That would *exceed* the recent FDA EUA tightening of 2 months median follow-up”; I think by “exceed” he means that Pfizer’s safety team would want to be slower rather than that they would want to be faster. He also says “the efficacy proof is lower than ideal” (i.e., we’d get better evidence by being less hasty), “the stakes here could not be higher. It’s our main exit strategy from the pandemic and we have to get it right” (i.e., he’s explicitly claiming that his motivation is to make sure that “we get it right”), and “That will help engender the public trust that is desperately needed. It will set the stage for high standards and success of multiple vaccine programs, which we also need. And the phenomenal science and velocity that got us to this point will not be put at risk.” (i.e., haste runs the risk of wasting all that hard work if it means the public doesn’t trust the vaccines that result).
(article text, initially quoting Topol) “Whether you are Pfizer, Johnson & Johnson, or Moderna, you want to win the race. But that is a different motivation than Trump has. He’s in a different contest,” says Topol. “Trump wants to win, but we need all the companies to win, because none can make enough vaccine [on] their own.” Any push to rush through a vaccine approval, in other words, would be motivated politically more than medically. Even though the pandemic is killing more than 600 people a day in the US, Topol doesn’t believe very much can be gained by declaring success a few weeks early. “We’re still going to be physical distancing and wearing masks after a vaccine. It’s not magic,” he says. “It’s more important that we get it right.”
I don’t really understand Topol’s argument in the first quoted bit. The article claims it means he’s worried that the push for quicker vaccine release is politically motivated, and that Topol is explicitly considering the tradeoff where faster release starts helping people sooner.
(article text) The White House had been holding up publication of an FDA recommendation that companies developing any covid-19 vaccine should search for side effects for at least two months in half their trial patients. [...] the FDA transmitted its recommendation to a key vaccine advisory committee, in what outside observers viewed as an end run past the White House. [...] But Topol believes Hahn and his deputies “stood up to Trump for the first time” and executed a “masterful” tactical maneuver.
Doesn’t say anything about Topol’s motivations, real or feigned.
That was rather long and tedious; my apologies. But the point is: Topol claims many times (and the article does, too) that Topol’s motivation was to do what is actually and visibly safe, and that the politically-motivated pressure was coming from the White House. Once again, of course he might have been lying, or he might have been motivated both by wanting the vaccines to be known to be safe and by wanting to deny Trump a political win. But, at least as far as this goes, it is simply not at all true that Topol said that his motivation was to deny Trump a political win. He said, over and over, that his motivation was to make sure the COVID-19 vaccines were known to be safe, despite (what he claimed to be) political pressure from the White House that put that at risk.
(For what it’s worth, my guess is that Topol genuinely believed that being slower about getting the vaccines authorized was better on medical and public-confidence grounds. And given what we actually saw with public confidence in the vaccines’ safety it’s not at all clear he was wrong about that. My guess is that he also much preferred Donald Trump not to get a political win. I don’t know what influence that had on his actions but, again, since his main argument was “if we rush these out then the public might not trust their safety” and what actually happened after they were not-quite-so-rushed out was that big chunks of the public didn’t trust their safety and many explicitly said that that was because they were rushed out, it seems like “he would have done the same even if he’d had no political motive at all” is pretty plausible.)
I oversold my original statement due to having remembered a slightly more sensational version of events. Nonetheless I stand by my interpretation of the tweets; others can read them for themselves and make up their own minde.
For those who don’t know and didn’t look these up:
NPI = Nonpharmaceutical Intervention Non-Pharmaceutical Interventions and COVID-19 Burden in the United States—PMC (nih.gov)
GDPR = General Data Protection Regulation What is GDPR, the EU’s new data protection law? - GDPR.eu
MAID = medical assistance in dying Medical assistance in dying—Canada.ca
Does this distinguish between IRL people and twitter clowns, or does it lump them into the same category? Twitter’s bots are around as good at using repulsiveness to shift people’s overton window as Trump is.
Weirdly, with the collapse of any externally imposed controls (lockdowns, mask mandates, vaccination requirements) and just general fatigue in the population at large, it’s become easier than ever to buy one’s way out of getting covid than it’s ever been. For instance, N95 masks are way cheaper—enough that I can switch them daily. With so few people getting the bivalent shot, I’m seriously considering going back for seconds.
>For instance, N95 masks are way cheaper—enough that I can switch them daily.
The pandemic showed me how useful masks are to have around, generally.
Cleaning that dusty room? Throw on my N95 and my allergies aren’t triggered.
Smoke from industry or wood stoves hanging in the air on a winter day, making my walk miserable? Oh right I have a mask in my glove compartment.
Sometimes I just use one purely to keep my face warm on a brutally cold day, if I didn’t bring something specifically designed for that.
Concerning MAID, if past trend are to be believed, the most terrifying thing is that these numbers will only get worse.
Is it terrifying because you think it’s bad if some people kill themselves with the program who otherwise wouldn’t have? Or is it terrifying that things are so bad in general that, once you give them more options, more will choose death?
If you mean the former – I really don’t share this judgment. Maybe you’re worried that sociopathic or act-utilitarian doctors will pressure patients – but these risks could be mitigated with safeguards, and they have to be weighed against the benefits (people being able to make informed choices about what they want and have their options increased).
If it’s the latter, then I agree. But I’m not surprised by this information, sadly.
Edit: And the same question to Zvi:
What does this mean? What’s the implication for policies you would push for? Should other countries try to install something similar or would that be terrible?
I guess it’s reasonable to be like “I don’t know, seems like a tough call and terrifying either way.” But there’s a risk that, if one feels an impulse to shy away from contemplating some topic in depth because it seems “terrifying,” it leads to biased opinions.