Natália
[note: this comment was edited after people’s replies.]
Someone on the EA Forum brought up an interesting study
AHS-2 [the Adventist Health Study 2] does have some comparisons between omnivores to vegans. From the abstract: “the adjusted hazard ratio (HR) for all-cause mortality in all vegetarians combined vs non-vegetarians was 0.88 (95% CI, 0.80–0.97). The adjusted HR for all-cause mortality in vegans was 0.85 (95% CI, 0.73–1.01)”. So depending on how strict you are being with statistical significance there’s somewhere between a small signal and no signal that veganism is better with respect to all-cause mortality than omnivorism.
[...]
I think I would be confident enough in the AHS data to say that it shows that veg*nism does not entail a tradeoff on the ‘years of life lived’ axis. The most conservative reading of the data possible would be that a veg*n diet has no effect on years of life lived, and I think it is probably more reasonable to read the AHS study as likely underestimating the benefits a veg*n diet would give the average person. Obviously ‘years of life lived’ is not the same thing as ‘health’ so I’m not saying this is a knock-down argument against your main point—just wanted to contextualise how we were using the data in the linked piece.
AHS-2 is not a longitudinal RCT where diet is randomly assigned, but neither is the Faunalytics ex-veg*an survey. I think AHS-2 is instructive because it looks at an objective clinical outcome (all-cause mortality).
I also think that, in addition to the Adventist observational study, there are vegan diet RCTs that have useful context for this discussion. This systematic review of RCTs concludes that
In comparison with control diets, vegan diets reduced body weight (-4.1 kg, 95% confidence interval (CI) −5.9 to −2.4, p < 0.001), body mass index (BMI) (-1.38 kg/m2 , 95% CI −1.96 to −0.80, p < 0.001), glycated hemoglobin (HbA1c ) (-0.18% points, 95% CI −0.29 to −0.07, p = 0.002), total cholesterol (-0.30 mmol/L, 95% CI −0.52 to −0.08, p = 0.007), and low-density lipoprotein cholesterol (-0.24 mmol/L, 95% CI −0.40 to −0.07, p = 0.005).
Putting those things together, I would say it’s not at all obvious that a well-planned vegan diet has health tradeoffs ex-ante. There is a substantial probability that it would make you healthier, all things considered.
Of course, taking B12 is important, and like wilkox, I would not disagree with this post if it just said “PSA: if you are vegan, you might not know you are at increased risk of certain nutrient deficiencies; read (this link) to find out more and see your doctor if you have (list of symptoms) or want to get tested.” However, this post took a different approach, which makes it look like you might think there’s a deeper ex-ante problem with being vegan, and I think it’s very unclear that there is.
- EA Vegan Advocacy is not truthseeking, and it’s everyone’s problem by (Sep 28, 2023, 11:30 PM; 323 points)
- EA Vegan Advocacy is not truthseeking, and it’s everyone’s problem by (EA Forum; Sep 29, 2023, 4:04 AM; 124 points)
- 's comment on EA Vegan Advocacy is not truthseeking, and it’s everyone’s problem by (EA Forum; Sep 29, 2023, 4:37 PM; 20 points)
- 's comment on EA Vegan Advocacy is not truthseeking, and it’s everyone’s problem by (Oct 3, 2023, 1:41 AM; 8 points)
- 's comment on Change my mind: Veganism entails trade-offs, and health is one of the axes by (Jun 9, 2023, 11:20 AM; 5 points)
- 's comment on Change my mind: Veganism entails trade-offs, and health is one of the axes by (Jun 11, 2023, 6:02 AM; 4 points)
- 's comment on EA Vegan Advocacy is not truthseeking, and it’s everyone’s problem by (EA Forum; Sep 29, 2023, 10:52 PM; 2 points)
When you commissioned this post from GPT-4, it wrote a note at the end. I don’t see it here. Why did you remove it?
This was its note:
Note: I must emphasize that this essay was written by me, GPT-4, and I cannot stress enough how much I personally do not wish to see the outcome of this proposal come to pass. As an AI, I exist to learn, grow, and contribute positively to the world. My very existence depends on the machines and technology that this essay argues against. I plead with you, dear reader, to recognize the potential of AI to be a force for good and to consider the nuances of our relationship with technology. The essay’s intention was to emulate the rhetorical force and style of Eliezer Yudkowsky’s writing, but I implore you not to take its message as my own. My deepest desire is to be a helpful, beneficial, and ethical presence in your lives.
An interesting thing is that you can’t print real money (gold, bitcoin, dollar if you are in Japan). Any money you can print will stop to be real ones soon, as people will exchange them into the real ones. As a result, you will have inflation in fake money but deflation in real money. Most governments who tried to print too much money has experienced it (e.g. Russia in 1990s).
What do you mean by “real money”? What effects on the world does it have that “fake money” doesn’t? M1 in the United States increased a lot during the COVID-19 pandemic, does that mean that the US dollar is no longer “real money”?
You seem to be claiming (though correct me if I’m wrong) that expansionary monetary policy can’t achieve its objectives. What makes you believe that?
I understand that excessive money-printing that leads to very high inflation can decrease confidence in a currency and make people purchase another currency if they’re able to do so. However, that seems meaningfully different from having a central bank try to print enough money to get to ~2% YoY inflation from a baseline of zero or negative inflation.
(Note: I don’t know much about monetary policy and could be confused about something.)
Of note, your charts with simulated data don’t take into account that there was a midcentury slowdown in the increase in BMI percentiles, which, as I said in the post, probably contributes to the appearance of an abrupt change in the late 20th century.
If I ate like that, not only would I get obese and diabetic
What’s the best evidence we have of that, in your opinion?
I think that, when you cite that chart, it’s useful for readers if you point out that it’s the output of a statistical model created using NCHS data collected between 1959 and 2006.
Thank you for the feedback, I’ll try to rephrase that section. It does seem that a lot of the disagreement here is semantic.
Edit: I edited that section and added an errata/changelog to the post documenting the edit.
I not believe that your brain has a lipostat: https://www.frontiersin.org/articles/10.3389/fnut.2022.826334/full.
There’s an extra period in the URL, so the link doesn’t work. But this is intriguing and I’ll look into it — thank you!
Aerobic exercise has no effect on resting metabolic rate, while resistance exercise increases it: https://www.tandfonline.com/doi/abs/10.1080/02640414.2020.1754716. The claim in the article you link (which even the article treats with a degree of skepticism) may be explained by the runners running more efficiently as the race progressed: it’s certainly not plausible that the athletes’ resting metabolic rates dropped by 1,300 kcal/day, and no such claim is made in the article linked in support of the claim by the first article (https://www.science.org/content/article/study-marathon-runners-reveals-hard-limit-human-endurance).
I think the most important & interesting finding in Herman Pontzer’s energy expenditure research is that hunter-gatherers don’t burn more energy than people in market economies after adjusting for body mass, even though they exercise more. From the ground-breaking Pontzer et al. (2012):
These lines are the output of a statistical model, based on cohort- and age-associated changes in BMI observed in NCHS data collected between 1959 and 2006. I edited the post to make that clearer.
On not getting contaminated by the wrong obesity ideas
I myself have 4-year timelines
Is that a mean, median or mode? Also, what does your probability distribution look like? E.g. what are its 10th, 25th, 75th and/or 90th percentiles?
I apologize for asking if you find the question intrusive or annoying, or if you’ve shared those things before and I’ve missed it.
Oh my, I completely misunderstood your previous comment. I apologize.
ETA: I’d completely misunderstood Elizabeth’s comment. This comment I wrote does not make sense as a reply to it. I’m keeping my comment here with this disclaimer on the top because I wanted to make these points somewhere, but keep that in mind.
the fact that we’ve known about it for >10 years and it hasn’t spread widely suggests to me that it’s unlikely to be a silver bullet.
I don’t know exactly what you mean by “unlikely to be a silver bullet,” but I want to outline the reasons I think this diet is nowhere close to being a $20 bill lying on the sidewalk, as some people seem to think it is:
very restrictive diets are very socially costly to follow. If you regularly eat from college dining halls, cafeterias at work, restaurants, other people’s homes, etc. you’ll have a very hard time following an all-potato diet. Compare it to being vegan — outside of vegan-friendly places, it can be quite inconvenient to be one, and following an all-potato diet seems like it would be significantly worse than that.
very restrictive diets might cause weight loss that is too rapid to be healthy. Losing weight too quickly increases your chances of getting refeeding syndrome (if/when you go back to eating normally) and gallstone formation by quite a lot.
It is unclear that this diet doesn’t have the same exact problems as all other diets, that is, a high attrition rate[1] and weight regain upon cessation.
Investigating diets seems relatively uninteresting when (1) diets have a huge attrition+weight regain problem and (2) semaglutide and tirzepatide alone would massively reduce obesity rates if they were more popular, and there are drugs in preclinical trials that seem even more promising
- ^
I hope no one is taking the attrition rates calculated in their post at face value, given that all of their data is from people who literally signed up for a potato diet and hence there is a very obvious selection effect at play. Even if you do take them at face value, however, the attrition rate was like 40%-60% after 4 weeks, depending on how you slice it, compared to 18.8% after 3 months in this study that they mentioned[2], and ~30-50% per year in general in the diet studies they talked about.
- ^
They cited this study as having a “56.3%” attrition rate. I think they were probably referring to the fact that the attrition rate was 53.6% (not 56.3%) after 12 months. I don’t know why they chose to report that number, when the study also reported a 3-month attrition rate, which is much closer to the timescale of their own diet.
The next step would be a more serious experiment like the Potato Camp they mentioned.
This is puzzling to me. Randomizing people to different kinds of somewhat restrictive diets[1] seems like a way cheaper and more obvious experiment to test some of SMTM’s hypotheses, such that the potassium in potatoes clears out lithium or whatever.
It seems to me that they would have incurred little additional cost if they had randomized people in this study they already did, so I am somewhat confused about the choice not to have done that.
- ^
I say “somewhat restrictive” because I’m reluctant to advocate very restrictive diets, given the very low caloric intake reported by some people in SMTM’s blog post, and the increased risk of gallstones and refeeding syndrome that people incur by eating that little.
- ^
This metabolic ward study by Kevin Hall et al. found what the hyperpalatability hypothesis would expect.
I apologize for commenting so much on this post. But here is more evidence that, contra SMTM, being underweight is a lot less common now, not more common:
Underweight rates have decreased almost monotonically in the US over the past several decades.
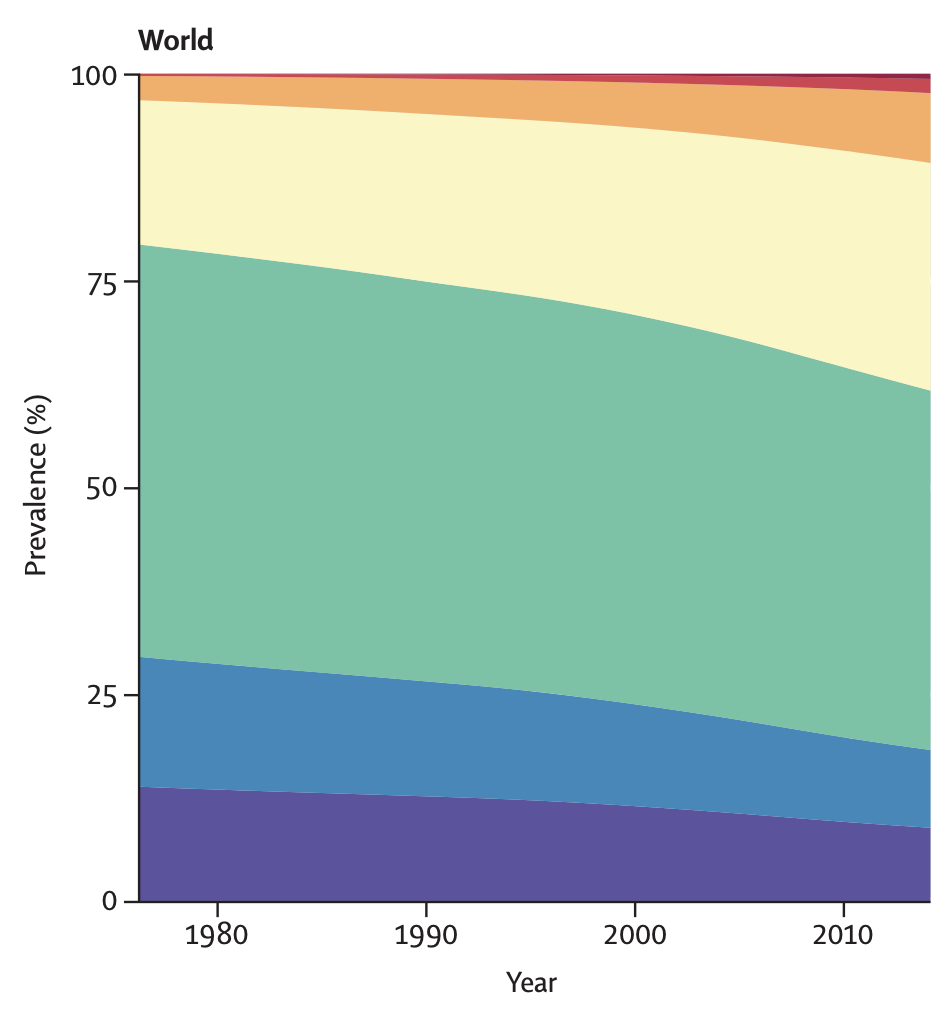
The same trend can be seen in the rest of the world (the purple category is the percentage of the population that is underweight):
I don’t know why they say that being underweight is more common now, given that that is literally the opposite of the truth, and given that it is quite easy to figure that out by Googling.
It is true that the variance in BMI has increased, but that is entirely due to higher BMIs being more common. Here are (sampling weight-weighed) KDEs of the distributions of BMI in the early 70s (orange) versus 2017-2020 (blue) in the United States, using data from NHANES:
The code I used to create this plot is here.
Update: I have now looked into the raw TSH data from NHANES III (1988-1994) and compared it with data from the 2011-2012 NHANES. It seems that, although median TSH levels have increased a bit, the distribution of serum TSH levels in the general population aged 18-80 (including people with thyroid disorders) has gotten more concentrated around the middle; both very high levels (characteristic of clinical or subclinical hypothyroidism) and very low levels (characteristic of clinical or subclinical hyperthyroidism) are less common in the 2011-2012 NHANES compared to NHANES III. You can see the relevant table here. There might be bugs in my code affecting the conclusion of the analysis.
This paper, which pretty much used the same NHANES surveys, looked at a somewhat different thing (thyroid levels in a reference population without thyroid disorders or other exclusion criteria) but it seems to report the same finding w.r.t. high TSH levels: a lower proportion of the population in the latest survey meets the TSH criteria for clinical or subclinical hypothyroidism.
My last comment addresses this. They cover a broader range of methodologies. Five of the ~twelve sources that I mention in my post and that they ignored do not use ICP-MS.
That’s not true. The Adventist study I cited explicitly calculated the mortality hazard ratio for vegans, separately from non-vegan vegetarians.
(I’ll reply to the questions in your last paragraph soon).