ProPublica came out this week with the best write-up so far of the full extent to which the FDA has been fighting to prevent us from having access to Covid-19 testing. Post is highly recommended.
We could have had lots of rapid tests early in the pandemic. Instead, many tests are still awaiting approval (aka they remain illegal) and we are facing massive shortages as people go around panicked trying to find a test.
Maddening non-sensical shifting standards and requirements are the FDA’s primary weapon, but simple inaction and delay are potent as well.
There’s a reminder of how the FDA did a similar thing with HIV testing and genetic testing, supposedly because of what might happen if someone got a positive test ‘without counseling.’
In the 1980s, the FDA banned home tests for HIV on the grounds that people who tested positive might do harm to themselves if they did not receive simultaneous counseling. In the 2010s, the agency cracked down on home genetic testing kits, concerned that people might make rash medical decisions as a result.
As opposed to what would happen if they didn’t get a positive test at all. I’m long past the point where I could consider this a well-intentioned mistake. There Is a War.
This is the conclusion, noting that missing a bar by 1% in FDA-land is also known as ‘missing a bar’ and ‘not better than having no test at all’:
And since rejecting Bosch’s submissions, the FDA has been coming around to her way of thinking. In March, the agency published a template for tests that would be used serially and sold in packages of two or more, allowing the kind of frequent testing she had advocated for. And last month, it published a new template that lowered the sensitivity standard for single-use over-the-counter tests to 80%.
Bosch had tests a year and a half ago that missed that bar by 1%.
For a while, even with the FDA’s attempts to stop it, as long as you were willing to pay about $10/test it was easy to get at-home Covid tests. Now that there’s need of them, that’s no longer the case. Stores across the city are sold out. Some places online still have tests, but Binex tests (which are the good ones) are extremely difficult to get, mostly sold out even at premium prices.

As a Buzzfeed report, note the contrast with how actual people talk:
Since our younger son’s last Covid test day at school, we went through an entire cycle of people getting low-level sick, doing rapid tests, and recovering, over the course of five days, before the tests from the school mostly came back. All were negative. There are similar reports from several other people I know.
It’s not only in America, things are completely out of hand.

We are also wasting a massive number of tests on children, who are required to get periodic tests ‘so they can keep going to school.’ They could go to school anyway, by… going to school. Or instead, we could double down on this waste of a limited resource, and focus what tests we have on school districts, as we are now doing in New York. I do appreciate the goal of not shutting things down on a single positive test, and if supply was abundant I’d be all for it, but it very much isn’t at this point and it’s only going to get worse for a while.
As always, make sure you know how to interpret your at-home test results.
Lines at Covid test tents keep getting longer here in New York, with most having dozens. The tests and their trucks do great work, but that doesn’t explain why we closed the testing sites at the airports. The return on testing capacity was always outstanding.
In San Francisco it seems things are also not so good (old news article about the closings).

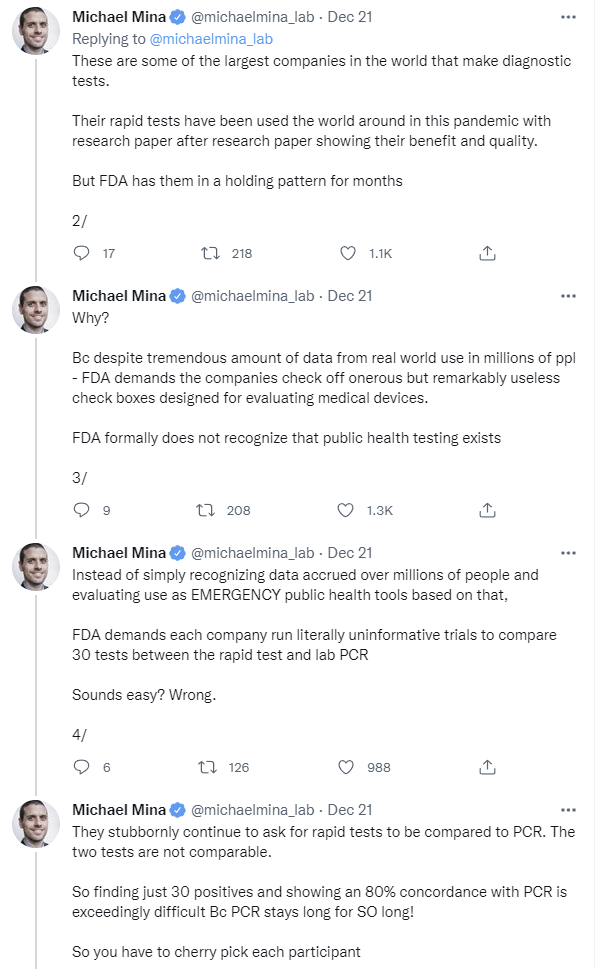
Why don’t we have more rapid tests? The biggest problem continues to be lack of approval for the tests, also known as the FDA making many sources of rapid tests illegal, using standards that make no sense. Here’s the metaphor version.
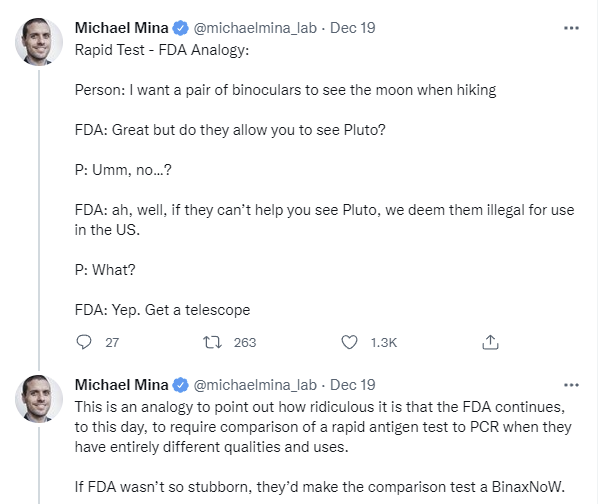
We could have hundreds of millions of additional tests, almost right away, including tests already used in Europe, if we simply made those tests legal. Here’s the more explicit version.
What is Biden going to do about this? No, he’s not going to put pressure on the FDA, let alone overrule them. That’s crazy talk.
He’s going to buy tests, that’s what he’s going to do, and send them to us. You know, send everyone in America a Covid test, no one’s press secretary would mock that excellent idea.
Alas, professionals talk logistics, and as has been the pattern for the Biden administration, actions are designed as symbols, and the logistics are a problem.

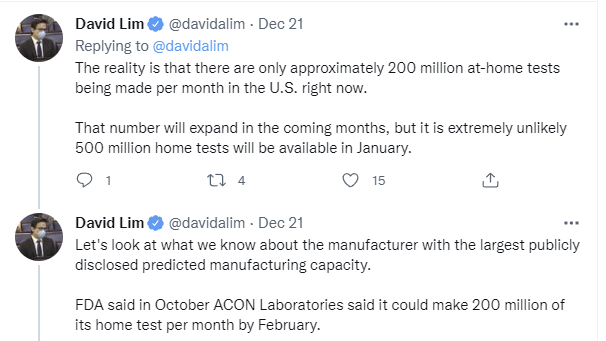
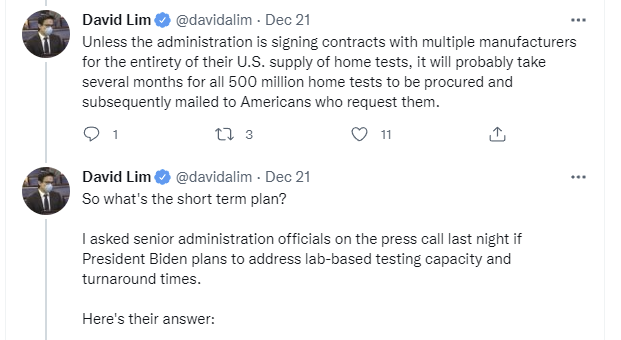
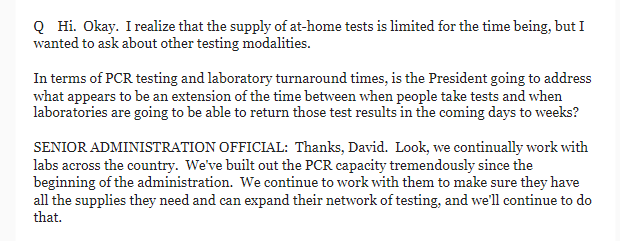
‘The supplies they need’ is not ‘the incentives they need’ nor is it ‘the regulatory permissions they need.’ Supplies are the kind of thing where Capitalism Solves This, if you fix the incentives and permissions. That’s not how these people think, and it shows.
Meanwhile, when testing is overloaded it slows down, because we’re unwilling to prioritize, which means all the tests become useless. You can’t know when to isolate, and you can’t get early interventions.

Making more Covid-19 tests legal would be a much more effective, and also much less expensive, way to get a bunch more tests. Instead, the tests Biden buys are coming out of our existing supply so they won’t arrive for a while, likely slower than they would have been given out anyway, and we won’t have more supply except on timescales of expanding manufacturing capacity. Except that with the Omicron wave likely over in a few months, and no advance commitments, who is even going to bother expanding capacity?
We also continue to not give robust guidance on how to use testing, and there’s every reason to believe a lot of testing over the holidays will be on the first day after exposure when tests won’t detect it yet. Even if Omicron’s generation time is down to two or three days, this window will still exist. With abundant tests this wouldn’t be a big deal, because we’d simply test again.
But if tests are hard to find, the supply must be rationed and one’s reserve conserved. Who is going to be able to test multiple times without symptoms? We wouldn’t even want them to do that right now. What should you do if your supply is limited, and you also don’t want to burn through too much of our collective supply, but you do want to stay safe and keep others safe?
Even more than everything else I write, not medical advice. But it looks like maximizing efficiency is about to be a lot more important. The biggest thing is to not test on the first day after a potential exposure. That’s a waste, a negative means little. Wait at least two days, and unless you have symptoms I’m guessing it’s better to wait until day three (isolating on day two to the extent you can) if you only get one test. And if you’re protected and aren’t going to expose anyone vulnerable, and you can’t easily restock tests or don’t want to hog them, maybe save your powder for when you have symptoms.
And remember why you had to do that.
FDA Delenda Est. But FDA not unique. We have it bad but so do many others. MR cites the example of Canada.
Here is what I take from your post:
Zvi: Allowing more tests at home would provide information. Information is good. The FDA should use lower criteria to allow more tests (and should have done that months ago)
FDA: Too low sensitivity and bad use of tests at home could lead to misplaced confidence. Misplaced confidence is bad.
Zvi: In this situation the extra information outweights the misplaced confidence.
FDA: In this situation the extra information does not outweight the misplaced confidence.
Can you provide evidence that the information indeed brings more value ? Also, did I miss the point of your post and/or misrepresent it ?
I guess my heuristic here would be looking to see if there are similar situations to the American situation in the world, and what they’re doing differently. Europe has quite a few similarities (EMA to FDA), (440 million to 330 million), and so I’d look to Europe for comparisons.
Anecdotally, buying a bundle of rapid tests in Europe was cheap and easy. They were available in every drugstore, and the ease/price of access was a huge advantage, which may be hard to overstate, especially if you’re coming from a position of “high” access to the American rapid tests.
(No easy ability to research these numbers at this time, apologies.)
Quoting half-remembered articles without sources, Europe hasn’t had higher numbers of super-spreader events. Europe hasn’t had significantly higher case numbers over the whole pandemic. Hard to think of what other statistics would show “extra information outweighing misplaced confidence”, but I feel that Europe has outperformed the US or been even with the US in the majority of those cases.
FDA is wrong. If tests are abundant, one can test every day and there is no problem of misplaced confidence.
The requirement for products to have the same cost/benefit profile really hampers innovation in the marketplace. A less sensitive test (literally, as a % of PCR) over the cumulative test-testing window (e.g., −2 to +5 days from symptom onset) may be desirable when used in a specific part of that window where it doesn’t actually have as severe of sensitivity disadvantage (e.g., −1 to +1 days). Depending on the disease, we may not want to compromise on specificity at all. These are just the “cost” profiles (haha I left out price) - the personal benefit is diagnosis (it’s the same whether it’s PCR or antigen).
But there is also a public health benefit to early diagnosis, which does differ across the tests (depending on test provider and logistical situation, this could be a 1 day vs. 15 minutes difference, or several(!) days vs. 15 minutes difference). Particularly in a situation where we’re trying to stop the spread of a disease that doesn’t need immediate serious treatment, a higher false positive rate may be acceptable (note: that means lower specificity, not lower sensitivity). This is why it makes sense to let a variety of products on the marketplace that meet a minimum threshold so the world can tradeoff along these various attributes (the FDA is charged with finding an appropriate quality floor, but that’s just a matter of dialing in the floor cutoff). Whether these tests will be prioritized by public health authorities (and the public) depends on the actual public health policy smorgasbord adopted and tastes among test properties.
So the FDA, inspecting these cost and benefit profiles, is not approving a test for diagnostic use based on its public health properties (which depend on the whole public health approach) and is instead looking at its personal diagnostic properties. Is the test not actually for diagnosis? That should certainly change the criteria. And I think, clearly, antigen tests are for diagnostic use. The goalposts of antigen vs. PCR testing are not different—“they test for different things” is a mischaracterization of what they do. They use different indicators but are testing for the same thing (COVID) to inform the same behaviors (which is also evident in how we’re talking about them as a substitute for PCR!). Notice that antibody testing uses yet a different indicator to test for a different thing (adaptive immune response) with different behavioral goals.
You may think the quality floor was set too high [I think so too, if that would have meant 80% sensitive tests in 2020 giving way to the 90% ones we see now, given the imperative of testing capacity] (or that quality floors shouldn’t exist at all, which is very delenda est) and generally the FDA has been too strict and slow in this emergency, but that’s not the same complaint as saying the FDA has been unfair or stupid on antigen tests in comparing to PCR.
The way antigen tests are used, they are frequently used to check whether or not someone is infectious when attending a given event on the day after the test was taken. If a person is infected but there’s only were little virus in their upper respiratory system, they aren’t infectious so it’s less problematic when the test doesn’t detect that.
I somewhat like the distinction between “testing for infectiousness” and “testing for whether I have it” (especially from a public health, rather than personal healthcare, standpoint). “People want to go to parties so they want fast, even if slightly less sensitive, tests because sometimes they don’t really even care about their own health status, just whether they can reasonably party” is also a great reason to try to market the product (let party organizers or other organization police what tests they will accept or whether they will expect pre-testing), but the FDA needs to assess that sensitivity somehow. What is the standard for infectiousness that the FDA is going to use to have a second evaluation pathway if there really is a distinction with a difference here? Probably some indicator of the amount of infectious virus present. A plaque assay (yields plaque-forming units, PFU) would be great, counting infectious particles, but the test itself takes days, needs BSL-3 conditions, and is resource intensive in other ways as well. Don’t compare to PCR, compare to PFU...that’s even more demanding against would-be antigen test manufacturers. And PFU has a pretty strong relationship with Ct. Compare to PCR then!
People are rightly dissatisfied with the status quo and looking for someone to blame for the lack of tests, but the problem is not that the FDA compares to PCR, it’s the threshold they wanted. I know “evidence-based decision-making” is abused and gets a rap, but I don’t think effectively advocating for evidence-less decision-making will make us less wrong (in case that sounds too harsh, what was the alternative to PCR that was supposed to validate antigen testing for us?).
The EU and the UK also have regulatory agencies that require evidence for accepting tests.
From https://ec.europa.eu/health/sites/default/files/preparedness_response/docs/covid-19_rat_common-list_en.pdf it seems that the alternative for using the straight comparison to PCR is:
That means that the test has to has a sensisitivty of 90% for patients with “Very high viral load”
The world is bigger then the US. In a case like this it makes sense to look at other countries who have enough tests for everyone who wants instead of just declaring the task impossible.
This is again a threshold, not comparator, complaint. Ct values are generated by PCR. Instead of using a crosstab for all samples, this approach is to use a crosstab for a subset of samples with higher viral load. It’s reasonable! IIRC from a previous paper, this (90% of Ct<25) has a similar effect as just reducing the overall cutoff to (80% of all). It’s also reasonable to use studies from other countries or to follow other agencies, in either case the ones we think are credible, which is again about the evidence threshold. What I’ve been hammering on is that the idea these tests are so different that they’re noncomparable is not sensible.