Things seem to have peaked in the Northeast once again. Nice.
Things are getting worse in the South as the summer hits. Not as nice, not that unexpected. At this point we can pattern match.
You know what else is nice? Not having to care about the pandemic. I do my best to care about it so you don’t (otherwise) have to, and hope to continue slowly dedicating less time and space to this each week. But for now, we continue.
You know what’s not so nice? A civilization that cares so little about an ongoing pandemic disease that its authorities refuse to authorize any spending, actively reallocate funds away from vaccine development, and otherwise do not take ordinary obvious steps to mitigate or solve the remaining problems. Also still technically having to mask up on the Subway and (for some reason) at my now go-to bakery.
You know what that’s still quite a lot nicer than? Being forced to care about the pandemic, and the destruction of massive amounts of value in prevention’s name for no meaningful gains. That sucked.
The general news is otherwise that we still don’t have any money for Covid, so Biden is shifting around what is left while it lasts, and the Moderna vaccine update works but we are unlikely to get it any time soon.
Executive Summary
Cases stabilize in Northeast, rising in South.
Moderna vaccine update is effective but FDA will stop it for a while.
Still no pandemic money.
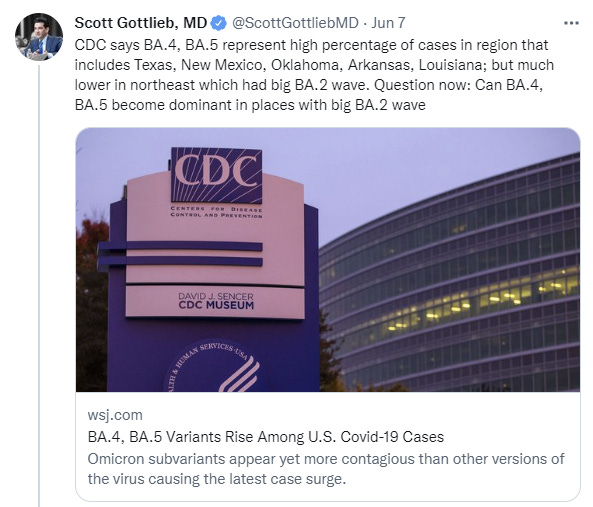
BA.4 and BA.5 taking over but it shouldn’t change things much.
Let’s run the numbers.
The Numbers
Predictions
NOTE: Florida numbers are cut in half because they report every two weeks (other half will count next week). North Carolina reported way too many deaths to not be a backfill, I subtracted 400.
Prediction from last week: 675,000 cases (+19%) and 2,400 deaths (+20%)
Results: 658k cases (+7%) and 2,220 deaths (+11%).
Prediction for next week: 700k cases (+7%) and 2,300 deaths (+4%).
Some aspects of CDC reporting are going down for 2 weeks for a system upgrade, the NVSS in particular. but they will continue to report death numbers. I am making predictions on the assumption that the numbers we see will not be impacted by this – if they are substantially impacted, that’s not what is worth predicting, so I’ll consider the predictions essentially voided. There is the horror of ‘a system upgrade should not shut down reporting for two weeks’ but we should probably be happy to be getting a system upgrade at all given what else we know.
Assuming reporting is normal, I expect the South to continue to have things get worse going forward due to the weather, but for things to otherwise improve. This is our new reality, and we’ll see the seasonal flows within that reality.
Deaths
[Deaths chart + graph]
Cases
How many cases are missing? We don’t know, but we do know it is a lot. Here’s a poll that provides some hints.
Some people actually do report these tests, but likely not the full ~25% listed here because the question was asked by someone in Medical Twitter, the group most likely to report. Even then, this was the top reply:
As far as I know, no one I know who has tested positive off an at-home test, and that did not require further treatment, reported the result. No one. If you did report your results, I’m curious to hear about what motivated you to do that.
We have this survey on who got it, keeping in mind this is a particular social group.
Of those who know they had it, how bad was it?
Lots more good stuff at the link.
The Guardian speculates that American cases may be thirty times the numbers being reported.
About one in five – 22% – of adult New Yorkers likely had Covid between 23 April and 8 May, according to the preprint study, which has not been peer-reviewed or published. That would mean 1.5 million adults in the city had Covid in a single two-week period – far higher than official counts during that time.
While the study focused on New York, these findings may be true throughout the rest of the country, Nash said. In fact, New Yorkers likely have better access to testing than most of the country, which means undercounting could be even worse elsewhere.
I am deeply, deeply skeptical that 1.5 million adults in NYC, 22% of its population, got Covid in a two-week period while placing zero serious strain on the hospital system, causing zero major disruptions and not causing a major spike in deaths. The number also does not remotely match my anecdotal experiences in the city.
But let’s suppose it is true. Is this bad news, as it is framed, or is it great news?
I say it would be pretty great. We know what the city looked like during those two weeks. It looked like New York City. The people lived like it was New York City. If Covid is now effectively so mild that a 1%+ daily infection rate risk doesn’t change anyone’s lived experience, how much higher can it ever possibly go? Why should we care about this at all?
BA 1,2,3,4,5
The version of Covid that replicates most successfully takes over, once again (CDC variant tracker).
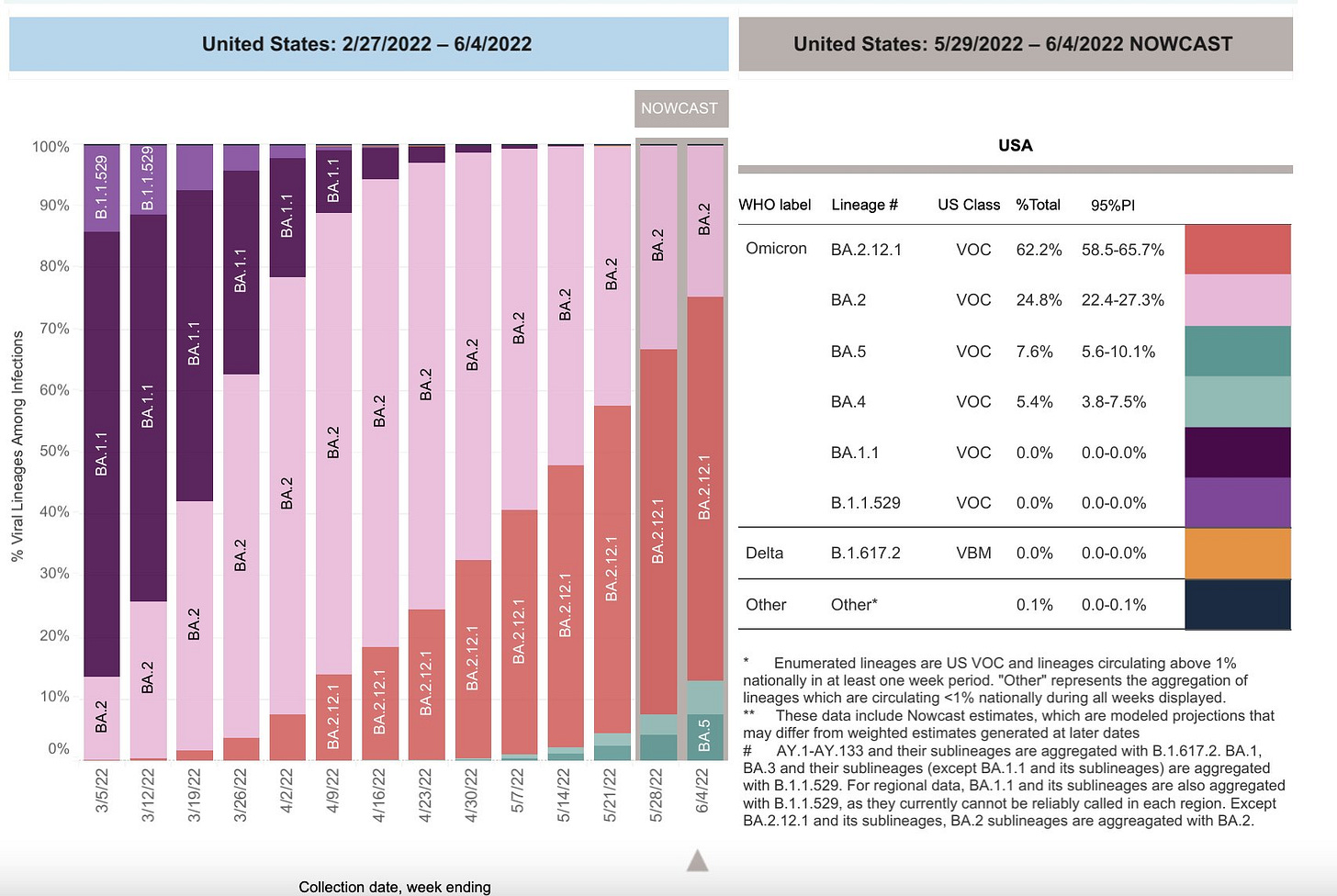
We do not need to wonder, BA.4 and BA.5 will become the primary strains unless something else comes along to challenge them, with BA.5 probably winning out but regional variation causes sufficient error in the data that it is too early to tell. By all accounts it does not much matter, and this should not worry us.
Often this is phrased as a question, as ‘will they take over?’
Technically it is a question, we can’t be certain, but I would not in any way think of this as the question, as it is neither especially high stakes nor is there much doubt what is going to happen.
Physical World Modeling
Introducing Taxonium 2.0, a tool for looking at lots of Covid-19 sequences.
Headline claims that used to sound absurd and now sound like Thursday:
It is important that this was an airport nail salon chain, XpresSpa, that always seemed empty whenever I passed it even before the pandemic. To survive the pandemic, they changed over to Covid surveillance, giving us data from airports and providing a potential model for future monitoring. This isn’t about taking samples from people while they got their nails done, or one particular heroic nail salon doing the bulk of our nation’s sequencing and surveillance. Not that I’d put it past us, at this point, to be relying upon a single airport nail salon somewhere, that sounds like the kind of thing we might do, but in this case it is thankfully not what happened.
Although the TV show about that salon would have been pretty cool. Think of all the colorful characters that could come through an airport nail salon each week. Nailed It is taken by a mildly amusing cooking show, so maybe Nailing Covid?
As is often the case, I found this useful for a different reason than the one offered (paper).
I don’t see how this provides the case for layered mitigation strategies – the case for mitigation depends on the ability of such an effort to meaningfully long-term succeed, rather than on pointing out that lesser efforts will often fail. But it is good to have the concrete 48% vs. 20% data point.
Still As Much Pandemic Funding As Sex in the Champagne Room
As in, none.
The Biden Administration is once again warning us about this and the resulting ‘unacceptable trade-offs’ it has to make with what little money is still left over, a situation that will only get worse without any new funds coming in. They are not only not putting money into but actively taking money away from vaccine development, in part to fund next generation vaccines that have already been developed in the hopes that the FDA will eventually make those safe and more effective next generation vaccines legal. Which it has not yet done, and may not do for a while.
These are indeed unacceptable trade-offs in the sense that they are not places we should be cutting funding, but also the practice of government and spending a budget is the practice of having not enough money chasing too many causes, and making trade-offs. This is an unacceptably horribly stupid situation, but to some extent I worry that what is being found most unacceptable to the mindset that often dominates is the very idea of trading off, of having to do A or B but not both A and B, because there is a class of ‘thing to be done’ that includes both A and B.
In this case, a reasonable class of ‘things that should definitely be done’ should definitely include A and B since their contents are things like ‘buy Paxlovid’ and ‘buy vaccines’ and ‘research vaccines’ but the number of things that many folks would put in the definitely pile is quite large and expensive.
The biggest thing being sacrificed seems to be at-home tests, which seems like the correct trade-off, with many of the freely provided at-home tests ending up mostly or entirely wasted, and this being the type of thing capitalism can easily solve, at least if the FDA permits it.
Besides, what do we use most at-home tests for? By mass of tests used, it is a combination of either wasteful periodic testing or slightly less wasteful prior-to-event testing. Often the periodic testing is an explicit punishment. For example, until this week the MTA was making the 23% of its workforce that didn’t vaccine gets weekly tests, presumably to try and force them to get vaccinated. That doesn’t seem like our top priority. Sending everyone free at-home tests while perhaps never getting additional Covid funds again seemed like a major unforced error.
The other potential major category is ‘give myself four or fourteen different tests after one exposure so I will feel slightly less nervous and no one will blame me for not testing often enough.’
There is a real category of ‘I actually needed to know if I had Covid’ but there will be plenty of tests for that.
Safe and Effective Vaccine Remains Illegal
The vaccine in question is Novavax. The good news is the situation is about to change.
Here is a live blog of the FDA hearing. Looked touch and go for a while.
After the hearing, the FDA advisory committee has unanimously recommended an emergency use authorization, so that is almost certainly going to happen soon.
The law governing emergency use authorizations (EUAs) by FDA requires that there is no “adequate, approved and available alternative” to a product. One advisory committee member asked Peter Marks, FDA’s top vaccine official, why the Novavax vaccine meets that requirement given that three other vaccines are already available to people in the United States.
“Having a protein-based alternative may be more comfortable for some in terms of their acceptance of vaccines,” Marks replied, noting that the law “allows us some leeway” to address unmet needs. “Anything we can do to get people … to be able to accept these potentially lifesaving medical products is something that we feel we are compelled to do.”
…
“I’m very skeptical that vaccine-hesitant people will elect to get this vaccine,” said committee member Jay Portnoy, an allergist and immunologist at Children’s Mercy Hospital. “Their hesitancy is more ideological than technological.”
But a parade of public speakers at the meeting mostly urged the committee to authorize the vaccine. “We need to … provide options to reduce excuses,” Martha Dawson, president of the National Black Nurses Association, told the advisers. “It could be the next thing that saves your life or your loved one’s life.”
How much of vaccine hesitancy is ideological and how much is technological? How much of it is ideological opposition to technology? How much is ideological sharing of conspiracy theories that have emphasized mRNA as a ‘dangerous’ or ‘unproven’ new technology, or raised some wild theory of what might happen with it? It has to be some mix of all of it, with substantial contributions from various sides.
I’d also see it as ‘an out’ for many people. If you get Novavax now, you can say you stood your ground, no one ‘forced’ you to do anything, you avoided the particular thing they were forcing on you, and all that. J&J couldn’t serve this purpose after public health decided to blow up that particular bridge, but now we get a redraw.
In practice, of course, I don’t expect this to become sufficiently top of mind for people to actually bother doing this all that often. But I think this will often be the true objection, that Covid-19 is over, no one cares, if you’ve made it this long what makes it worth bothering to do this now?
Novavax’s vaccine is also easier to store, so it has two advantages and could still make at least some difference even here. The storage advantage is a much bigger advantage in less developed countries.
Another thing we heard from the hearing is that while Novovax also occasionally does get associated with Myocarditis, cases associated with either Novavax or mRNA tend to be much milder than viral cases. 2% ICU level support versus 50%(!) for viral cases, 12% Cardiac dysfunction vs. 60%, hours to days recovery time versus days to months. This is not remotely the same thing.
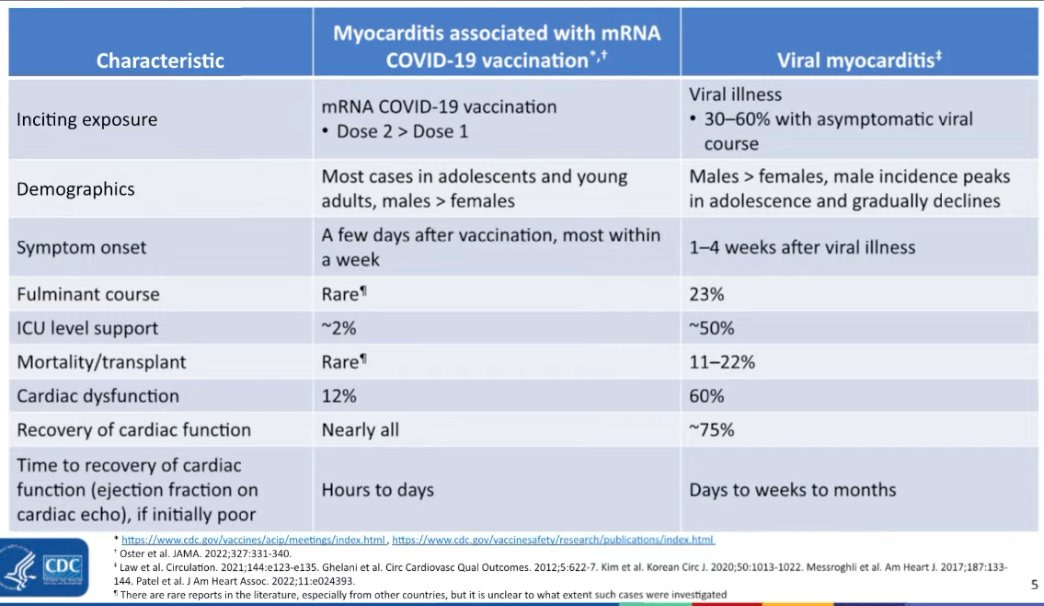
That could be because there isn’t a causal link to the vaccine, and the whole thing is phantoms.
More Effective Version of Moderna Vaccine Remains Illegal
The good news is that it works and is a large improvement.
The bad news is that this ‘working’ involves putting shots of the new vaccine into arms, and it is highly unclear there will be any of that happening any time soon.
“The data are definitely better than I had even hoped,” Burton told ABC News that in an interview. “Given the magnitude of effect — that seven-fold increase in antibody levels — we could for the first time, be at a vaccine that is truly effective with once yearly dosing because we know those antibody levels will decay.”
…
Moderna plans to file its data with the Food and Drug Administration “as quickly as possible,” and should the vaccine be authorized, the company will be ready to supply the shots to “as many people around the world as possible,” Burton said.
It is not what we hoped in 2021, but it is far better than we hoped back in 2020, and as a worst case option it is highly acceptable at this point.
On the front of quickly updating the vaccine for new variants, however, this has already been a stunning failure compared to what is possible given the technology. The attempt to spin this into a success on that front is strained at best.
Should another variant of concern emerge, one drastically different than omicron and the already existing variants, scientists at Moderna will be prepared to reevaluate and readapt the shot to address the new threat.
“If something again really drastic occurs, Well, we’ll have to look at that. But I would say again, what I think we’ve been able to show here, is that we can adapt very quickly. We were able to make this new booster in weeks and get it into testing. I think we can even speed that up now. So, I think we were well prepared for that,” Burton said.
This is weeks to get it into testing. That is not quite useless, but when it counts it won’t be good enough. Months after there are enough infections from the new variant to properly ‘test’ the new vaccine and get the show on the road will very much be after the resulting wave peaks. If we are facing a truly bad new variant, a vaccine update will not save us, because our Public Health Authorities have zero interest in finding a way to make the timeline work.
Here is Chise analyzing the results in a thread with the technical specs.
So no question it is a substantial improvement. Again, it is not perfect, but it is what we could have reasonably hoped for at this stage.
The problem is that the FDA is about to meet to decide what should go into the new formulation.
As in, no, they are not going to simply allow Moderna, some random pharma company, to decide what goes in their vaccine and then decide if it’s a good update. Instead, the FDA is going to decide what the update looks like.
And what happens if the FDA’s update proposal is slightly different from what Moderna tested, in the months in which the FDA did not decide what it was going to mandate?
That’s right. Moderna would likely have to run all the tests over again, because different things are different, and we are not allowed to have priors. So that would be another several months of delay, and ensure that we would not have an updated vaccine for the fall. Which is what seems most likely to happen.
It is a good thing we don’t have to care about this pandemic.
Don’t Worry About the Monkeypox
Not that no one should be worried about the Monkeypox, but you, on a personal level, in terms of you changing your behaviors to avoid getting it?
I get that question every so often, so here’s public health reminding us what it is all about.
Yes. Exactly. It is always, always, always possible to make your plans a little safer. You can change your plans. You can make them otherwise worse, so they will be a little safer. Then you can change them again, and make your plans worse again, and they will again be a little safer, unless your first change was to cancel your plans.
To the extent that you have a good cost-benefit on bothering to do the cost-benefit on that, you should do the cost-benefit on that, and occasionally make changes to your plans.
But most plans should absolutely not need to give non-zero amounts of thought to summer colds or food poisoning or monkeypox.
Who should be worried about monkeypox on a personal level, at all? If you are MSM, and taking multiple partners who in turn have multiple partners, then yes, you should consider altering your plans. To suggest to everyone else that they should be considering whether to change plans, which a large portion of people I know have had to stop to consider, is pure innumeracy. That considering and freaking out has a real cost, including exhausting people’s freaking out capacity and/or increasing their freak out capacity, both of which are best avoided.
If you are tempted to take foolish precautions that sacrifice life lived for little gain, perhaps we should tell you about racial disparities in public health. As MR tells us, talking about such disparities decreases fear of Covid and decreases support for interventions, which makes sense since it points out that your risk and the risk to those around you is lower than you thought. The biggest inequality, of course, is based on age rather than anything else, and is an even better thing to keep in mind.
It could always be worse, things could be justified by pointing to us still taking shoes off at airports, as if that made safetyism look good.
Think of the Children
Don’t get me wrong. My kids are vaccinated and I do think vaccination is very worthwhile. But does this show the importance of raising vaccination rates in kids? (paper)
It is certainly useful information, but the importance of raising vaccination rates in kids also depends not only on how much this translates to actual risk of reinfection, on the importance of preventing reinfections in kids. How much should we care?
I am inclined to think that we should care exactly to the extent that those kids infect others and thus alter the equilibrium of the epidemic, but to care almost exactly zero about the kids themselves. These are reinfections, among a group where even first infections among the unvaccinated pose miniscule risk.
When deciding whether to vaccine my kids, I definitely wasn’t thinking about whether it would protect against them getting Covid a second time.
In Other News
Paper on how bad epistemics caused deaths during the pandemic.
Mina thread on why T-cells are so important.
A model of Covid as a five stage disease (paper) with Long Covid as the fifth stage, based on a review of papers. I am not convinced but seems worth passing along.
A (quite correct) call to use American Rescue Plan funds to improve air quality via HVAC systems, which has a variety of strong benefits.
Long thread from Bloom Labs about what we know about the origins of Covid.
Not Covid
With potential grain shortage worldwide, Biden increases mandatory amount of ethanol to go into gasoline. This could end very badly.
But some of that gas will go into driverless taxi services in San Francisco. Nice.
I’m, personally, quite interested in finding a way to make the timeline work. I’m also quite interested in making the timeline work for preventing infection with the current circulating variants. Then we can start on the common cold.
Is the plan around here to actually listen to the public health authorities on this? Or is something being organized to route around these sorts of regulatory failures? (For example, by manufacturing and distributing up-to-date vaccines within a state only, to keep them out of interstate commerce.) Nobody working on RaDVaC seems to have yet been arrested; maybe doing more of that and trying to make it more accessible to non-microbiologists would be more better?
Or is the potential gain in terms of coronavirus cases and deaths prevented by faster action not going to be worth the cost of annoying the relevant authorities, plus the cost of doing the actual work, plus the risk of doing it wrong?
Just wear a respirator and be done with it.